

Parkinson’s disease, or “PD,” is a neurodegenerative disorder of the central nervous system. PD is predominantly diagnosed in elderly patients, but 5% of cases happen to patients less than 40 years old. Parkinson’s disease affects more than 6.1 million people worldwide, and patients diagnosed with primary parkinsonism can be characterized by non-motor and motor symptoms. Some patients with vascular parkinsonism or white-matter disease need a separate review of neurovascular conditions such as CSVD, because the treatment discussion is different from idiopathic PD.
Breakthrough Therapy for Parkinson’s with Stem Cells
Several types of stem cells are currently being used to treat Sporadic PD. Some of the stem cell-derived therapies have only been studied in clinical trial settings and have been used in Parkinson’s and other neurodegenerative diseases. These stem cell-based therapies include:
- Embryonic Stem Cells (ESCs): These can potentially turn into any cell type in the body. There have been concerns about the ethical implications of using ESCs, and there is the potential for tumor formation when implanted. The Regeneration Center does not offer human embryonic stem cells for Parkinson’s disease.
- Induced Pluripotent Stem Cells (iPSCs): These are cells taken from adults and reprogrammed to act like embryonic stem cells. This technique sidesteps the ethical concerns of using embryonic cells; however, it poses a risk of developing cancers because the IPSC cells can insert DNA anywhere in the cell’s genome, which can trigger the expression of cancer-causing genes. The Regeneration Center does not offer induced pluripotent stem cells (iPSC) stem cell replacement therapy for Parkinson’s
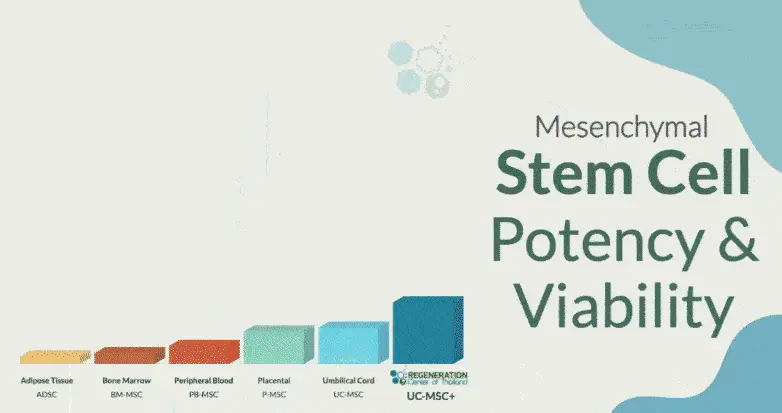
- Isolated Mesenchymal Stem Cells (UC-MSC+): Found in several tissues, including bone marrow, cord tissue, placental tissue, dental pulp (neurogenic), and adipose tissue. Isolated UC-MSC Cells have been successfully used to treat many diseases due to their anti-inflammatory properties. Patients with advanced Parkinson’s disease have limited options when it comes to stem cell sources. The Regeneration Center offers isolated and expanded mesenchymal cells that can home and differentiate into any cell type, including stem cell-derived midbrain dopaminergic neurons.
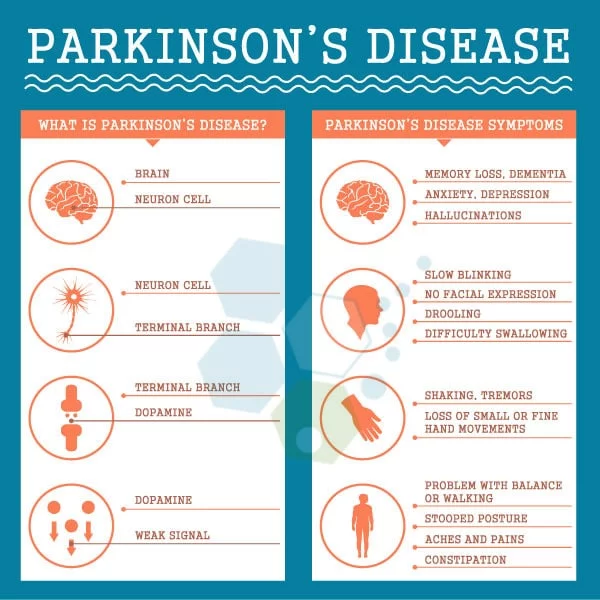
Common symptoms of Parkinson’s Disease (PD)
The disruptions caused in motor control often include:
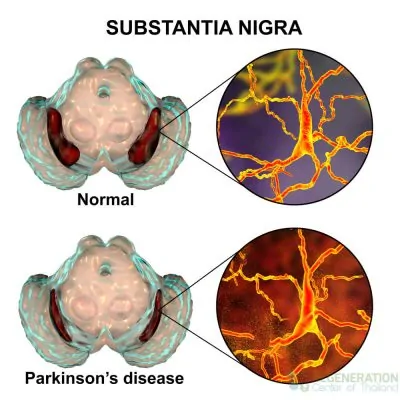
- Mild Tremors ( Typically when over 65% of dopamine neurons have degenerated in the substantia nigra.
- Slowness in movement ( bradykinesia )
- Muscle rigidity, movement dysfunctions, and a reduction in dopamine-producing cells
- Poor Posture, Motor Function, or Postural Instability
History of Parkinsons Disease & Paralysis Agitans
In 1817, a British physician named James Parkinson described in his treatise “An Essay on the Shaking Palsy” the main symptoms of the disease, which was later named after him. Other names and classifications in the Parkinson’s disease family include:
- Shaking Palsy
- Idiopathic Parkinsonism
- Parkinson’s syndrome
- Corticobasal Degeneration (CBD)
- Drug-induced Parkinsonism
- Vascular (Arteriosclerotic) parkinsonism or Multi-infarct parkinsonism
- Progressive supranuclear palsy (PSP)
- Hypokinetic–rigid syndrome (HRS)
- Essential Tremor (ET)
- Paralysis Agitans
What Causes Parkinson’s Disease
For most patients (Over 85% of all cases), the diagnosis of Parkinson’s disease is idiopathic or of unknown origin. Researchers studying Parkinson’s believe that it may be caused by several factors, ranging from systemic autoimmune diseases and genetic/familial causes to environmental causes. Familial Parkinson’s is quite rare, and less than 15% of our patients have reported a family history of Neurodegenerative disorders such as ALS, Ischemic Strokes, Broca’s aphasia, or Ataxia. The primary pathophysiology of Parkinson’s disease is the death of dopaminergic neurons (dopamine-producing cells) and motoneurons in the midbrain (substantia nigra region). The typical symptoms associated with PD result from the loss of paracrine signaling by neurotransmitters, particularly dopamine. Some other potential risk factors for neurodegenerative diseases like MND and PD include oxidative stress, autoimmune system complications from disorders such as lupus, hereditary variables, environmental factors, neuroleptics or calcium antagonists, intoxication (Drug-induced parkinsonism), or traumatic brain injuries.
[1]
Is Parkinson’s caused by genetic mutations?
While the risk is low, several genetic mutations can lead to the development of Parkinson’s disease in some individuals. These include mutations in genes such as:
- SNCA – Alpha-synuclein gene
- PRKN – Parkin RBR E3 Ubiquitin Protein Ligase
- PINK1 Gene PARK6
- DJ-1 and PARK7 Gene
- LRRK2
It is believed that mutations in these genes can cause dysfunction and eventual death of dopamine-producing neurons through various mechanisms, including protein aggregation, mitochondrial dysfunction, and oxidative stress. The most common genetic mutation found in patients with Parkinson’s disease is in the LRRK2 gene. However, having one of these mutations does not necessarily mean that an individual will develop Parkinson’s disease; there are likely complex interactions with environmental and other factors. Though only a subset of Parkinson’s cases can be attributed to genetic causes, identifying these mutated genes has provided essential insights into the underlying biology of the disease. This could eventually help lead to more targeted and effective treatments. Further research is still needed to fully understand all the genetic contributors to Parkinson’s disease, and the Regeneration Center offers full genetic screening for Parkinson’s and other neurodegenerative diseases.
The Role of Lewy Bodies & Symptoms of Parkinson’s Disease
A diagnosis of PD is given when a patient develops a rapid accumulation of alpha-synuclein proteins into the “Lewy bodies” due to the inadequate activity of neurons and dopamine. Dementia with Lewy bodies is reported as the third leading cause after Alzheimer’s and vascular dementia. The four primary symptoms of Parkinson’s disease are bradykinesia, rigidity, tremors, and postural instability.
What is Bradykinesia – Bradykinesis?
Bradykinesia refers to a patient’s slowness of movement and inability to change position. Activities and motor functions, such as rising, walking, and turning, can be challenging. Sometimes, for patients with late-stage Parkinson’s, voluntary movement is almost impossible due to akinesia.
The first sign of PD disease may be that an arm resonates less when walking. Due to frontal gait disorder, the patient’s posture is often flexed, and turning may require multiple intermediate steps. Gestures and facial expressions decrease; a patient’s face usually looks emotionless, like a mask. The voice becomes quieter and monotonous, and language skills become more indistinct. The person has difficulty eating and often chokes. The handwriting becomes small and illegible.
Limitations of Dopamine Antagonists & Managing Rigor
Rigor describes the stiffness of the muscles. Every movement appears to face fierce resistance. The neck and shoulder muscles are often affected, typically on one side. A neurologist may be able to detect the Cogwheel phenomenon. An example of cogwheel rigidity is observed when a physician attempts to stretch the patient’s arm with Parkinson’s disease, resulting in jerky movements as if a cogwheel were turning.
Rest tremors
Resting tremors, or tremors at rest, often occur in patients with Parkinson’s disease, typically on one side. The slow tremors of the hands and, later, the feet occur primarily during rest periods. The resting tremors often disappear during exercise or sleep. How do you cure brain fog? The tremor is absent in all cases, but many patients report empty hands and fingers rubbing against one another in a movement resembling “counting coins.”
The Role of Physical Exercise & Postural Instability
Postural instability is a primary motor symptom in a later stage of shaking palsy. The lack of balance is particularly apparent when the patient stands upright. PD directly affects the reflexes that help us balance, and patients with postural instability can easily fall with the slightest touch. This symptom is very dangerous for patients and often leads to severe falls, resulting in orthopedic injuries to the hips, knees, shoulders, and arms.
Parkinson’s disease and movement disorders
Parkinson’s disease is a progressive neurological disorder characterized by tremors, stiffness, slow movements, and balance issues. It is caused by the death of dopamine-producing neurons in the substantia nigra region of the Brain. Other joint movement disorders include dystonia (sustained muscle contractions that cause abnormal postures), chorea (involuntary, jerky movements), tics (sudden, rapid, recurrent motor movements or vocalizations), and restless legs syndrome. Movement disorders can significantly impact the quality of life. A multidisciplinary approach that includes neurologists, physical therapists, occupational therapists, speech therapists, and mental health professionals is essential.
What are some Complications of PD: Akinetic Crisis?
An akinetic crisis (AC) or acute akinesia is a life-threatening complication of PD that can be caused by a variety of issues, including infections, medication errors, or failed surgery. A patient with AC becomes completely immobile, can no longer speak, and can no longer swallow. Accompanying symptoms include sweating and a fast pulse. Such a crisis is dangerous and must be treated immediately. Without the ability to swallow, saliva can enter the lungs and cause pneumonia.
Onset of Parkinson’s & Early stages of the disease
When someone aged between 18 and 50 years old receives a clinical diagnosis of Parkinson’s, it is called young-onset Parkinson’s disease or early-onset Parkinson’s disease. The symptoms of PD are usually the same regardless of age, but younger patients have very different experiences with the condition due to their age. From a psychological, social, and medical standpoint, managing PD is challenging for younger patients and their families.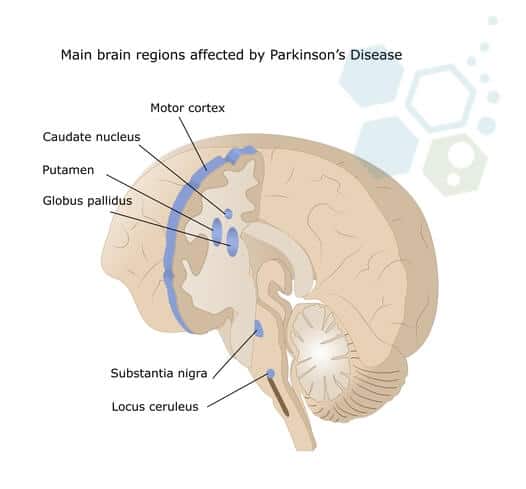 Early symptoms and accompanying symptoms for the onset of Parkinson’s disease include:
Early symptoms and accompanying symptoms for the onset of Parkinson’s disease include:
- The sense of smell worsens.
- Sleep disorders associated with involuntary and violent movements during REM sleep (REM sleep behavior disorder)
- Frequent depression and unhappy moods
- Diffuse muscle pain, reduction in motor function, and pain in the shoulder-arm areas (due to muscle stiffness and limited mobility)
- Excessively oily skin due to hyperactive sebaceous glands in the face
- Issues with body temperature and circulatory system regulation
- Problems with proper bladder and bowel function
- Reduced Cognition
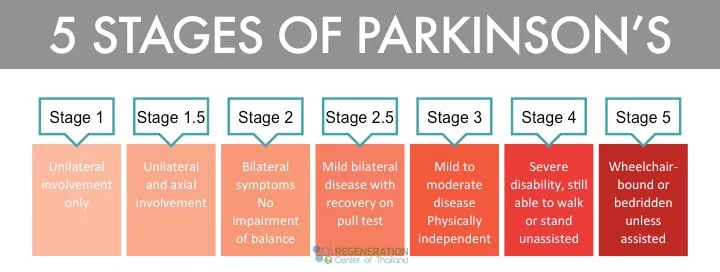
5 Stages of Parkinson’s Disease
Symptoms of Parkinson’s vary from person to person and can take a while to manifest, and the disease is regarded as slow-moving or “insidious onset.” Early symptoms include neuropathy, tremors, and clumsy movements, even at rest. Severe symptoms include muscle rigidity, bradykinesia, and gait disorders. Other non-motor symptoms include incontinence, depression, insomnia, and astriction. Neurologists have established the Hoehn and Yahr Scale, which consists of the five stages of PD to help classify patients in clinical trials and research studies worldwide.
Diagnosis of Parkinsonian Syndromes
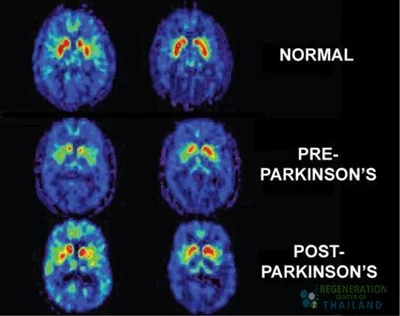
Diagnosis can be challenging, but patients we have treated at the regeneration center for PD generally don’t show significant abnormalities in lab panels or blood tests. Still, trained neurologists can usually detect irregularities in Cerebrospinal fluid biomarkers through radiography tools such as brain MRI or CT Scan.[2]
The symptoms of Parkinson’s are progressive, but each patient shows a different rate of progression. Loss of motion function is associated with a decline in overall quality of life, and drugs have shown minimal efficacy in clinical trials and in treatment worldwide. For severe cases, traditional medicine has virtually no impact and can make it even more challenging to control the symptoms due to new side effects. Severe patients often demonstrate catalepsy and can develop other complications, such as lung respiratory failure, Parkinson’s disease psychosis, and Parkinson’ s-related hallucinations.
Pharmaceutical-based solutions are ineffective for symptomatic patients and cannot alter the course of the degenerative disorder. Drug-based treatments cannot raise the number of neuron cells, thus making most of the traditional treatment options ineffective.
Genetic Testing for Parkinson’s
Hereditary neurodegenerative diseases occur when genetic mutations are passed from the parents to their children. A genetic disease, however, may result from environmental factors or heredity. Random mutations can cause genetic conditions in the DNA due to environmental factors or exposure to toxins. Familial (hereditary) PD accounts for less than 15% of all confirmed cases. Inherited Parkinsonism is either an X-linked dominant pattern or an autosomal recessive pattern. Each parent carries one copy of the mutated gene but often shows no signs or symptoms. For this reason, autosomal recessive PD can frequently be misdiagnosed as dementia with Lewy bodies, multiple system atrophy (MSA), or ALS/MND. The most common genetic markers used for screening hereditary Parkinson’s include LRRK2, Glucocerebrosidase (GBA), RIC3, PARK2, PARK6, PARK7, SYNJ1, PTRHD1, TMEM230, UCHL1, DNAJC6, CYP2D6, VPS13C, PODXL, DNAJC13, CHCHD2, and RAB39B. Recent research also suggests that abnormalities in tau proteins are a potential cause of familial Parkinsonism and frontotemporal dementia.[3]
The Regeneration Center offers gene sequencing tests for 18 of the most common genetic causes of Parkinson’s disease and monogenic Parkinsonism-related conditions. The genes we can test for include: SLC6A3, LRRK2, DNAJC6, FBXO7, GCH1, PARK7, VPS35, PINK1, PRKRA, PRKN, SNCA, SPR, TH, CHCHD2, MAPT, ATP13A2, ATP7B & DCTN1
Please note we do not offer gene therapy for Parkinson’s disease, but offer gene testing services for existing patients looking to confirm a diagnosis or who are displaying classical signs of Parkinsonism and can benefit from molecular diagnostic testing. The panels offered by the Regen Center cover genes with recessive, dominant, and X-linked inheritance patterns, clarifying recurrence risk and identifying which relatives may be at risk based on family history.
TREATMENT RISKS & PRECAUTIONS
Please note that not all patients are suitable candidates for treating Parkinson’s Disease with stem cells. Patients with advanced motor symptoms, severe cognitive decline, or other significant health conditions might not be good candidates for treatment. The Regeneration Center does not offer embryonic stem cells or induced pluripotent stem cells for the treatment of Parkinson’s diseaseTreatment Options for Parkinson’s in 2026
Parkinson’s disease and some of its symptoms are treatable, but a cure for Parkinson’s using gene therapy is not available. Recent developments in gene editing and exosome therapy do offer hope for a potential treatment for Parkinson’s. However, the research remains in its infancy and has not yet proven consistent. Traditional therapies for PD consist of several components to counter low levels of dopamine neurotransmitters in the Brain, with the most common one being pharmaceutical medications. Anti-Parkinson medications are effective for some patients, allowing the disease to be under control for many years. Over time, however, the effect of new Parkinson’s drugs may decrease. Therefore, frequent medication adjustments are necessary at specific intervals to ensure that treatments remain effective.
The most common medications for Parkinson’s Disease include: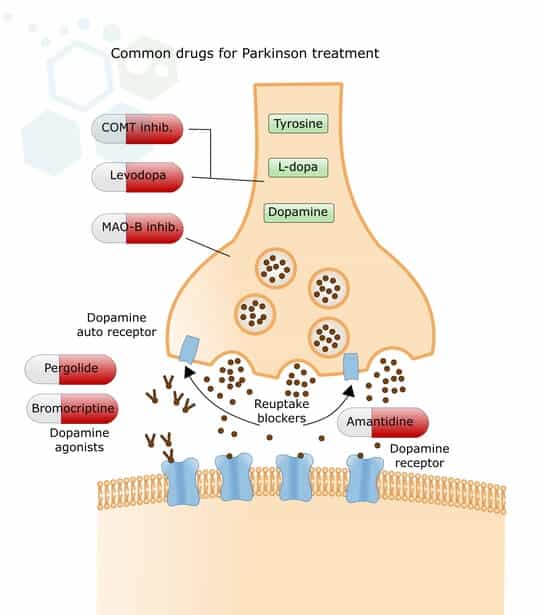
- Levodopa (L-DOPA) is a dopamine precursor that helps nerve cells absorb it and convert it into dopamine. L-DOPA has positive effects on mobility, muscle stiffness, and tremors. However, after a long period of L-DOPA therapy, results can cause a variety of side effects, including hyperkinesia (unpredictable and uncontrollable movements) and on-off phenomena. To counteract fluctuating efficacy in advanced stages of Parkinson’s disease, some patients have an internal dopamine-producing pump that delivers dopamine continuously via an implanted probe into the small intestine or under the skin.
- Carbidopa-levodopa (Sinemet)—This new medication combines carbidopa and levodopa. This more modern medication can prevent levodopa from degrading in the gastrointestinal tract and help reduce adverse effects, such as nausea.
- Dopamine Agonists – This group of PD medications mimics the effects of dopamine on brain cells, causing neuron cells to react to them precisely as they would to natural dopamine. These medications also increase the impact of the existing dopamine (pramipexole, lisuride, ropinirole). Newer forms of dopamine agonists ensure consistent, even drug levels throughout the day. They must be taken in part only once daily (extended-release ropinirole, extended-release pramipexole) to increase dopamine levels. These medications can also deliver the active ingredient via a dermal patch, which must be changed daily (Description: Rotigotine patch). Side effects of dopamine agonists may occur in the form of daytime fatigue or drowsiness, and the form of compulsive behavior, such as compulsive purchasing and gambling addictions.[4]
- Other groups of medications can help reduce the effects of dopamine (COMT inhibitors such as entacapone and tolcapone) or slow down its breakdown (MAO-B inhibitors such as selegiline and rasagiline).
- Anticholinergic agents (E.g., Biperiden, Bornaprin) can effectively reduce tremors and movement disorders.
- NMDA inhibitors, such as amantadine, can help to increase dopamine release and improve mobility for some patients with damage to the substantia nigra pars
Is there a cure for Parkinson’s Disease?
For advanced Parkinson’s disease cases, some doctors also recommend using dopamine agonists and different groups of active ingredients with each other. Still, this approach is challenging because each medication’s symptoms and side effects can vary, leading to unexpected responses when combined. Current clinical trials of stem cells have limitations, but stem cell research has shown promising results in halting disease progression. Isolated neural stem cells can differentiate into dopamine-producing neurons lost in Parkinson’s disease. Preliminary clinical trials used neurons derived from pluripotent stem cells; however, the researchers injected these neurons into the brains of patients with Parkinson’s disease, resulting in complications. The Regeneration Center employs the latest stem cell technologies and advances in stem cell manufacturing to treat the disease and improve motor function, with a lower risk than using IPSC cells. Our ongoing research focuses on the most effective methods for differentiating stem cells into neurons, the optimal stem cell types to use, and the optimal delivery mechanisms. While there are still significant challenges to overcome, the future of stem cell therapies and neural stem cell therapies offers an exciting alternative treatment not just to manage symptoms but also to slow or stop the progression of Parkinson’s disease via dopamine cell replacement.
Deep Brain Stimulation (DBS) & Surgical Interventions for PD
For some patients with Parkinson’s who do not respond well to medication, they may be offered brain surgery as a treatment option. There are very few surgical options for treating conditions like MS & PD, but the most common one is called deep brain stimulation (DBS). DBS involves surgically implanting a device in the Brain that generates electrical impulses via a battery-operated neurostimulator. The results of DBS are not very effective over the long term and carry a lot of risk due to the need to perform surgery on a patient who is already sick. Given this risk, doctors and patients must weigh the potential benefits against the risks, and programmed pacemakers in the Brain should be used only when drug therapy is no longer effective.
Stem Cell Treatment for Parkinson’s
In Parkinson’s disease, specific nerve cells die in the Brain. Clinical trials worldwide aim to develop a new cure for Parkinson’s by replacing dead neural stem cells with dopaminergic neurons and neurotransmitters. One idea was to take stem cells from the bone marrow and implant them in the Brain (stem cell injection, stem cell transplantation). According to the theory, stem cells in the patient’s mind should differentiate into new, functional nerve cells, or at least compensate for deficits, in people with Parkinson’s disease.
This approach sounded promising, but transplantation of bone marrow stem cell lines did not always lead to the desired results and was ineffective, resulting in potential harm to the patient. Since the development of adult stem cell therapy, new methods have been developed to replicate/replace diseased cells using isolated and expanded mesenchymal cells (UC-MSC+). Neural stem cells have proliferative activity in specific adult brain regions, particularly in the subventricular zone and hippocampus. These cells can differentiate into various neural cell types, including neurons and glia, but typically do not generate large numbers of dopamine neurons in the cortex.
Long-term effects of stem cell therapy for Parkinson’s Disease
We are still in the early stages of regenerative medicine, and the long-term effects of stem cell therapy for Parkinson’s disease are still largely unknown. Initial treatment outcomes have been promising, with patients showing increased dopamine cell counts and modest improvements in motor symptoms that persisted for up to 2 years after treatment. The actual test of stem cell therapies for Parkinson’s will be whether cell transplants can provide sustained dopamine production and related symptom relief over many years.
What are the side effects of stem cell therapy?
Long-term safety and misuse of stem cell delivery methods also need careful evaluation, as there are valid concerns that the types of cells used may develop into tumors or cause other adverse effects over time. The Regeneration Center is committed to multi-year longitudinal studies to better understand the durability of improvements, optimal cell doses and delivery methods, and any delayed risks. Once proven safe and effective over the long term, stem cell therapy will modify the course of Parkinson’s disease, providing lasting regeneration of dopamine neurons and significantly improving quality of life.
Culturing Neurons & Neural Progenitor Cells
The dopamine-producing cells used in the treatment are first isolated from regions of neurogenesis. The multipotent stem cells require culturing (expansion) over several days to differentiate them into functional astrocytes, neurons, and oligodendrocytes. The Regeneration Center’s proprietary treatment protocol to treat movement disorders like Parkinson’s using neural stem cells is built on the latest advances in stem cell technologies and cell manufacturing.
Mesenchymal stem cells for Parkinson’s
The Regeneration Center uses isolated stem cells that may be unique, as they target the central nervous system to enhance motor neuron function and improve overall quality of life. The therapy for people with Parkinson’s also focuses on the underlying mental symptoms via infusions of progenitor cells that can release dopamine, which then raises the levels of new neuron cells needed to slow down, stop, or, in some cases, reverse the gradual progression of Parkinson’s before it’s too late.
Stem Cell Therapy for Memory Loss
The Regen Center Stem Cell Therapy for Parkinson’s enables targeted, customizable delivery of dopamine-producing cells to induce neurogenesis across multiple stages, depending on the patient’s underlying health status. The treatments are effective in being absorbed by the tissues after crossing the blood-brain barrier through cerebrospinal fluid or a nebulizer.[5]
Treatment options for movement disorder & Parkinson’s using Stem cells w/ dopaminergic neurons may include:
- Radio Guided Therapy
- The stereotactic technique of deep-brain stimulation
- Striatum stereotactic pallidotomy
- Subarachnoid stem cell implantation via lumbar puncture
- Brain cell stereotactic operation – Stem PD
Implanted neural stem cells support dopamine transport channels and eventually differentiate into dopaminergic neurons, thereby maintaining healthy & functional neurotransmission. We use isolated Mesenchymal stem cells for treatment (UC-MSC+). These cells differentiate into nerve cells, including dopamine-producing and dopamine-agonist cells. The quantity & types of implanted cells (growth factors) depend strictly on the medical needs of Parkinson’s disease patients.
Physiotherapy Management for Patients with Parkinson’s Disease
Physical therapy cannot reverse or stop Parkinson’s disease. Still, such treatment options can help improve a patient’s independence and overall quality of life by enhancing cardiovascular health, strength, range of motion, and pain relief. Good physiotherapeutic care is essential for maintaining mobility for as long as possible. Speech therapy can also help patients with impaired language and swallowing. Non-verbal communication via gestures and facial expressions should also be encouraged whenever possible.
Occupational therapy and psychological care also help families and caregivers cope independently with everyday life and engage in hobbies as they typically do. A professional therapist can help sufferers and families deal with the mental health problems or symptoms the patient might be experiencing.
Parkinson’s Diet: Foods to Eat and Avoid
While there is no single Parkinson-specific diet to maintain good health, most patients with PD should be more cautious than most by eliminating junk food and trying to maintain a balanced diet full of antioxidants (vegetables, fruits, and dark chocolate), whole grains, dairy fat, and protein-rich foods such as legumes and meat to boost dopamine levels. Lifestyle diets such as the Mediterranean diet and ketogenic diet can positively influence both motor and non-motor symptoms of patients with Parkinson’s, reduce systemic inflammation, and increase dopamine-producing cells.
Stem Cell Treatment for Parkinson’s – 2026 Guidelines
The goal of stem cell therapy for Parkinson’s disease is to alleviate the patient’s symptoms and restore any lost neurological function. The treatment is performed on an outpatient basis, and cell transplantation is performed noninvasively. Stem cell treatment for PD may not be a good option for all cases, so we request that potential patients submit recent medical diagnoses, lab results/CT scans to our medical team for review.
If you would like to learn more about how functional medical therapies can be applied to treat Parkinson’s Disease or have any other questions, please contact us.
Published Clinical Citations
[1] ^ Agosta, Federica, Ammar Al-Chalabi, Massimo Filippi, Orla Hardiman, Ryuji Kaji, Vincent Meininger, Imaharu Nakano, et al. 2014. The El Escorial criteria: strengths and weaknesses. Amyotrophic lateral sclerosis & frontotemporal degeneration, no. 1-2 (December 8). doi:10.3109/21678421.2014.964258. https://www.ncbi.nlm.nih.gov/pubmed/25482030
[2] ^ Naujock, Maximilian, Nancy Stanslowsky, Peter Reinhardt, Jared Sterneckert, Alexandra Haase, Ulrich Martin, Kwang-Soo Kim, Reinhard Dengler, Florian Wegner, and Susanne Petri. 2014. Molecular and functional analyses of motor neurons generated from human cord-blood-derived induced pluripotent stem cells. Cure for Parkinson’s with Stem cells and development, no. 24 ( 15). doi:10.1089/scd.2014.0180. https://www.ncbi.nlm.nih.gov/pubmed/25007389
[3] ^ Phanthumchinda, K, O Supcharoen, and E Mitrabukdi. 1996. Madras pattern of motor neuron disease: case report from Thailand. Journal of the Medical Association of Thailand = Chotmaihet thangphaet, no. 6. https://www.ncbi.nlm.nih.gov/pubmed/8855616
[4] ^ Sarlak, Golmaryam, Anorut Jenwitheesuk, Banthit Chetsawang, and Piyarat Govitrapong. 2013. Effects of melatonin on nervous system aging: neurogenesis and neurodegeneration. Journal of Pharmacological Sciences, no. 1 (August 27). https://www.ncbi.nlm.nih.gov/pubmed/23985544
[5] ^ Terashima, Tomoya, Hideto Kojima, Hiroshi Urabe, Isamu Yamakawa, Nobuhiro Ogawa, Hiromichi Kawai, Lawrence Chan, and Hiroshi Maegawa. 2014. Stem cell factor-activated bone marrow ameliorates amyotrophic lateral sclerosis by promoting protective microglial migration. Journal of Neuroscience Research, no. 7. https://www.ncbi.nlm.nih.gov/pubmed/24936617