
Renal Cancer, also known as Renal cell adenocarcinoma (RCC) or Kidney cancer, is a group of cancers that start in the kidneys. Symptoms of renal cancer can include lumps in the abdomen, blood in the urine, or chronic back pain. Other symptoms can include rapid weight loss and fever. Kidney cancer is diagnosed when oncologists find abnormal cell growth in the kidney tissue. Over time, these cells form a tissue mass known as a tumor.
Kidney cancer can begin when something in the environment triggers a change in renal cells, causing them to divide uncontrollably. If a malignant or cancerous tumor can spread to other tissues or vital organs, it’s called metastasis. Kidney cancer can metastasize to several organs, including the liver, lungs, or brain.
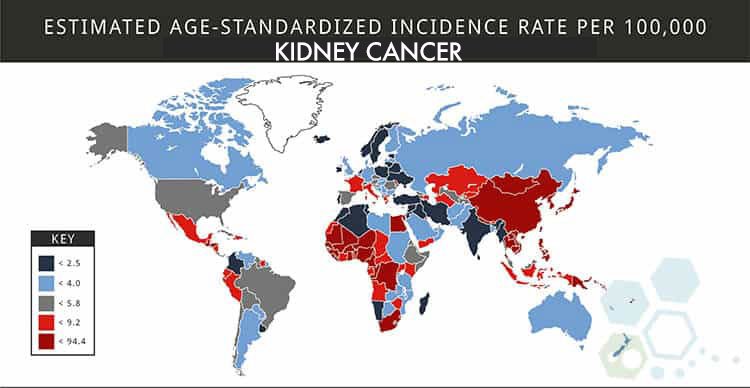
Global Kidney Cancer Statistics
Based on recent statistics from 2021, Renal cancer is the ninth most commonly occurring cancer in men and the fourteenth-most common cancer type in women. The total number of patients with renal cell adenocarcinoma has nearly tripled since the 1980s. There is an increasing global trend in the incidence of kidney cancer globally, particularly in younger populations and European countries. Doctors have identified several modifiable risk factors for developing kidney cancer. The rapidly increasing incidence of kidney cancer amongst young individuals is quite worrying and requires early intervention with active preventive measures.[1]
Those most susceptible to developing kidney cancer include People between the ages of 65 and 74, who have the highest incidence of developing kidney cancer, and the prevalence of the condition in men is two times that in women. Additionally, Native Americans and people of African descent are disproportionately affected. In contrast to adults, children seldom get kidney cancer. However, every year, between 5000 and 6000 children are diagnosed with Wilms tumors, a rare kind of kidney cancer.
Types of Kidney Cancer
There are many kidney cancer variations, and each type is quite different in the way it develops and mutates over time. Treatment options vary depending on the type, scale, and severity of the diagnosis. The three most common types of renal cancer include:
Renal cell carcinoma (RCC)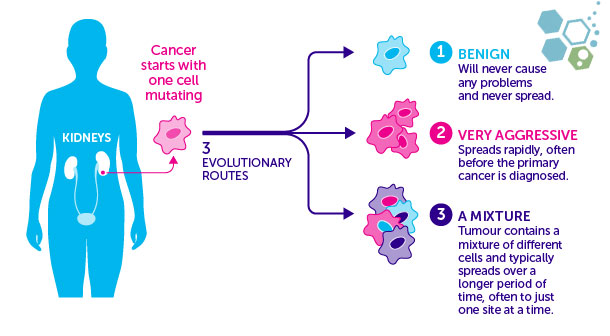
RCC is the most common form of kidney cancer in the world. RCC is responsible for 85% of all kidney malignancies and is the most frequent kind of kidney cancer in adults. While renal cell carcinoma most often manifests as a solitary tumor in just one kidney, it can also spread to other organs and is usually seen in patients with chronic liver disease and alcoholic liver cirrhosis. Cancer develops in the tubular epithelium that lines your kidneys (tiny tubes that return nutrients and fluid to your blood). Clear-cell renal cell carcinoma (RCC) accounts for most cases (ccRCC).
Transitional cell carcinomas
Six to seven percent of all kidney malignancies are transitional cell carcinomas. Uterine carcinoma typically develops at the point where the ureter branches off from the kidney proper. Your renal pelvis is the place where your kidneys are located. The ureters and bladder are potential sites of progression for transitional cell cancer. [2]
Renal sarcoma
Renal sarcoma is extremely rare, making up about 1% of all instances of kidney cancer. This disease originates in the kidneys and can spread to other organs and bones if left untreated. Renal sarcoma forms in the connective tissue surrounding the kidneys or the adipose fat around the kidneys. Less than 1 percent of identified kidney cancers are classified as renal sarcoma, and the location of kidney cancer pain can vary depending on stage.
Wilms tumor
Wilms’ tumor is commonly a type of renal cancer in children. Wilms’ tumor is also known as nephroblastoma and most often affects children from the ages 3 to 5 but becomes much less prevalent after the age of 5.
How Common is Renal Cancer?
About 9.7% of all malignancies are diagnosed as kidney cancer. On average, around 566,000 people are diagnosed with kidney cancer each year, and renal cancer is more likely to be diagnosed in older people. In its early stages, kidney cancer may not cause any symptoms. Yet, signs and symptoms may emerge as the tumor develops. This is why kidney cancer is frequently not identified until it has already spread to other organs.
Metastatic renal cancer – Secondary kidney cancer
 When cancer is found in the kidney, it might not have developed there but has metastasized (spread) from bone cancer or other organs, resulting in prostate cancer, colon cancer, lung cancer, pancreas cancer, stomach, prostate cancer, or breast cancer. Since this type of cancer has spread from another (primary) site, it is referred to as secondary renal cancer. The tumors are classified and treated according to the primary site of origin. For example, cancer that begins in the pancreas and spreads to the kidney is referred to as pancreatic cancer and not kidney cancer. It is also treated like pancreatic cancer. In North America & Europe, secondary (metastatic) renal tumors are more commonly diagnosed than primary kidney cancer. Still, the opposite is true for many parts of Asia (Thailand), South America, and Africa.
When cancer is found in the kidney, it might not have developed there but has metastasized (spread) from bone cancer or other organs, resulting in prostate cancer, colon cancer, lung cancer, pancreas cancer, stomach, prostate cancer, or breast cancer. Since this type of cancer has spread from another (primary) site, it is referred to as secondary renal cancer. The tumors are classified and treated according to the primary site of origin. For example, cancer that begins in the pancreas and spreads to the kidney is referred to as pancreatic cancer and not kidney cancer. It is also treated like pancreatic cancer. In North America & Europe, secondary (metastatic) renal tumors are more commonly diagnosed than primary kidney cancer. Still, the opposite is true for many parts of Asia (Thailand), South America, and Africa.
Benign Kidney Tumors
Sometimes, the tumors found in the Kidneys are classified as noncancerous (benign). This type of cancer usually doesn’t cause any severe symptoms or discomfort. Benign renal tumors are often found by chance when a patient undergoes imaging tests for other health conditions. Common benign tumors in the kidneys include:
- Renal adenoma – Adenoma on the kidneys is one of the most common benign kidney tumors. They are typically small, low-grade growths.
- Renal oncocytomas are benign (asymptomatic) tumors that can grow large. They can develop throughout the body and are not unique to kidney tissue.
- Hemangioma
- Cysts and polycystic kidney disease
- Fibroma – Fibromas are also tumors on fibrous tissue surrounding the kidneys. This type of cancer is rare and more common in women.
- Lipoma—Lipomas are renal tumors that originate in the fat cells in the renal capsule or surrounding tissue. They usually occur in middle-aged women.
- Angiomyolipomas, also known as angiomyolipomas or renal hematomas, are typically benign tumors caused by familial genetic mutations. This diagnosis can be isolated but is often associated with the genetic disease known as tuberous sclerosis. Patients with tuberous sclerosis can develop tumors in the prostate, skin, liver, brain, colorectal, and other vital systems.
Symptoms of kidney cancer
- Uterine bleeding (hematuria)
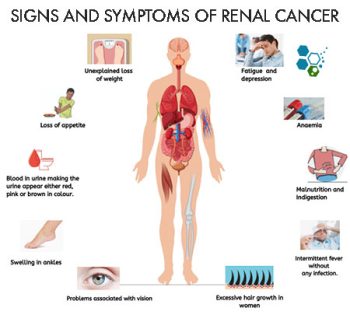
- You have a mass near one of your kidneys
- Experiencing aches in the flank
- Frequent tiredness or brain fog
- A pervasive malaise, an absence of health
- Disturbance in regular eating habits.
- Rapid weight loss
- A persistent mild fever
- Abnormally high blood pressure
- Anaemia
- Significant amounts of calcium
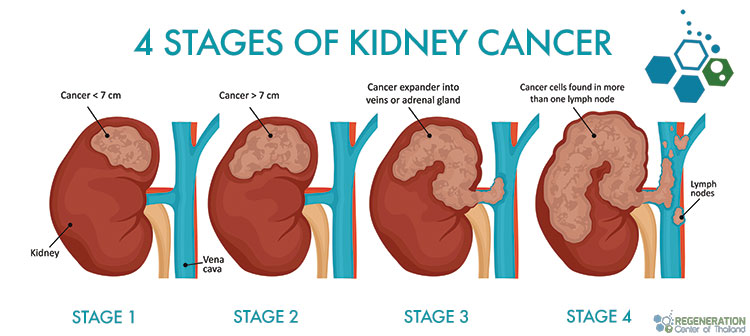
The Four Stages of Kidney Cancer
An essential part of dealing with kidney cancer is classifying it into one of four stages. This facilitates planning for appropriate treatment based on stage and severity. The stage of renal cancer will be based on several factors, including staging and diagnostics, to determine which stage is inaccurate.
There are essentially four primary stages:
- Stage 1 kidney cancer: Cancer has not spread to any other organs, is localized in the kidneys, and is smaller than 7 cm in diameter
- Stage 2 kidney cancer: Cancer has not spread to any other organs and is localized in the kidneys, but is more than 7 cm in diameter
- Stage 3 kidney cancer: Cancer might be any size and has spread to nearby organs outside of the kidneys
- Stage 4 kidney cancer: Cancer has spread from the kidneys and metastasized to distant locations, including lungs, lymph nodes, brain, bones, and liver.
What Are Lymph nodes?
Lymph nodes are like little “filters,” collecting and storing white blood cells that may be used to fend against infections. To measure the level of dysfunction in a patient’s lymph nodes and the size of tumors, a doctor utilizes radiology scans such as CT and MRI, along with biological samples (via biopsy) from tumors, to establish the extent of the disease.
Grades are assigned to tumors to reflect how their cells deviate from normality. Grading can also estimate the rate of tumor growth. High-grade tumors are characterized by rapidly dividing abnormal cells that don’t resemble healthy tissue. It is common for high-grade tumors to develop and spread faster than low-grade ones.
Diagnostic tests for kidney cancer
To reach a diagnosis, an oncologist looks through a patient’s medical history records and does a preliminary physical examination, looking for signs of kidney cancer. They may also request tests to aid in the detection and evaluation of cancer. Indicators that may be used in such examinations are:
- Urinalysis – Urine samples are used to check for the presence of blood. Urine tests can identify even the tiniest amounts of blood that would be undetectable to the human eye.
- Blood tests check electrolyte levels and count blood cell types. Reduced red blood cell count (anemia) and renal disease are detectable with a simple blood test (by looking at the creatinine levels).
- A computed tomography (CT) scan is an X-ray technique that uses a computer to produce multiple cross-sectional images of the body. Intravenous contrast is commonly used in this examination (dye), and Dye administration may be unsafe for those with compromised renal function.
- Cystoscopy scans allow doctors to see inside a patient’s body through a skinny, flexible tube called a.
- An MRI scan uses a powerful magnetic field to create images of the organs and structures deep within the human body.
- An ultrasound scan can examine the body to produce pictures on a screen by sending high-frequency sound waves into the tissues. Tumors have a different density from healthy tissues; thus, this test can assist in their detection.
- A renal mass biopsy entails inserting a tiny needle into the tumor and removing a tissue sample (biopsy). A pathologist can examine the tissue sample under a microscope to determine whether cancer cells are present. Your doctor may or may not prescribe a kidney biopsy because of the test’s limited accuracy in detecting cancer.
- Renal Arteriogram. This test is used to evaluate the blood supply to the tumor. It is not given often, but it may help diagnose small tumors. It has other uses, as well. [3]
Kidney Cancer Prevention & Risk Factors
Major risk factors associated with cancer in the kidneys include: 
- History of acute renal injury or kidney disease
- Family history of kidney cancer. This risk is very high in siblings
- Smoking tobacco
- Alcohol abuse
- Obesity
- History of High Blood Pressure (Chronic Hypertension)
- Being on long-term dialysis
- Exposure to environmental toxins or chemicals such as cadmium, asbestos (mesothelioma), organic solvents, benzene, and broad-spectrum herbicides.
Having any of these risk factors does not mean you will automatically get kidney cancer. It’s also possible that patients can have none of these symptoms but still get the disease.[4]
TREATMENT RISKS & PRECAUTIONS
Please note that not all patients are suitable candidates for treating Kidney Cancer with Immunotherapy, CAR-T, or NK Cell therapies. Patients with advanced metastatic disease, severe organ dysfunction, or other significant health issues might not be good candidates for treatment.Treatment Options for Kidney Cancer
When a patient is diagnosed with kidney cancer, oncologists first try to determine if the cancer tumors have spread and, if so, how far. They can then use the patient’s cancer stage and current health status to discuss the most appropriate treatment options with the highest likelihood of survival. From there, treatment selection is typically guided by a few core variables: tumor stage (localized vs locally advanced vs metastatic), tumor size and location within the kidney, histology (most commonly renal cell carcinoma), overall kidney function, and the patient’s performance status and comorbidities. Imaging (typically contrast CT or MRI of the abdomen/pelvis, plus chest imaging) helps define the extent of disease, while biopsy is sometimes used when the diagnosis is uncertain or when systemic therapy is being considered before surgery. This initial workup also clarifies whether the tumor is amenable to curative local therapy or whether treatment needs to focus primarily on long-term disease control.
Surgery for Kidney Cancer & Kidney Tumors
Surgery is still considered the first option for treatment for benign kidney tumors or non-metastasized kidney cancer. Laparoscopic surgeries offer minimally invasive surgery and require only small incisions in the patient’s abdomen. Doctors can then insert a small camera and other medical instruments to target and destroy the tumor. Recent clinical trials have shown that laparoscopic surgery is equally effective as previous surgery but allows for a much easier recovery.
Other types of surgeries for renal cancer include:
- Robotic Partial Nephrectomy – In a partial nephrectomy, only the affected kidney area is removed.
- Minimally Invasive Urologic Surgery
- Radiofrequency Ablation – In Ablation surgeries, extreme temperatures target and kill cancer cells. In radiofrequency ablation, a needle is inserted into the kidney tumor from the outside. The next step is to destroy the cancer cells by applying an electric current across them. Cryoablation and radiofrequency ablation are common alternatives to surgery that may help certain people.
- Cryoablation – Doctors puncture the skin, inject liquid nitrogen, and remove the tumour from the kidney. Cold gas is then used to freeze the cancer cells.
- Laparoscopic Radical Nephrectomy—During a radical nephrectomy, both kidneys and part of the tissue around them are surgically removed. Lymph nodes around the affected area could also be removed. After a kidney is lost, the goal is for the healthy kidney to assume the functions of the failing one.
Active Surveillance – Small Kidney Tumors
Doctors often employ a strategy called “watchful waiting” or “active surveillance” for certain patients with tumors, mainly when the cancer is slow-growing, minor, or asymptomatic. This approach involves closely monitoring the tumor for abnormal growth or changes over time without immediately resorting to treatment such as surgery, radiation, or chemotherapy. Regular  imaging tests, including CT scans or MRIs, are used to assess the tumor’s size, location, and characteristics to track its progression.
imaging tests, including CT scans or MRIs, are used to assess the tumor’s size, location, and characteristics to track its progression.
Transitioning from active surveillance to more aggressive treatment depends on several critical factors. The patient’s age is considered because younger individuals may tolerate more intensive treatments better and have a longer life expectancy, making long-term outcomes a crucial consideration. The patient’s overall health also plays a vital role, as those with other severe health conditions may face higher risks from invasive treatments and may benefit from delaying or avoiding them.
The size and location of the tumor are key determinants, as tumors in sensitive or vital areas of the body might require earlier intervention due to the risk of complications. Tumors that are growing near critical structures like blood vessels or nerves, or in places where they could obstruct organ function, may necessitate prompt treatment even if the cancer appears slow-growing. Lastly, the rate of growth observed over time is a significant factor. A tumor that remains stable for months or years may be managed under surveillance; however, if imaging reveals increased size or changes in tumor characteristics, a more proactive treatment plan may be required to prevent further complications.
Ultimately, active surveillance aims to balance the benefits and risks by avoiding unnecessary treatments when the tumor remains stable and acting decisively when there are signs of progression. This individualized approach helps patients maintain their quality of life while mitigating the risks posed by the tumor.
- Patients age
- Patient’s overall health
- Size and location of tumor – Via imaging (CT, MRI)
- The overall growth rate of a tracked tumor over time
Immunotherapy Kidney Cancer in 2026 – RCC therapy
Biologic-based therapies, such as NK Cell Therapy, also known as Immunotherapy, are a new type of kidney cancer treatment designed to enhance the body’s defense mechanisms to fight cancer. mRNA technology and Biological therapies can use autologous materials (generated by the patient’s body) or allogeneic materials (cultured in a laboratory) to target, restore, and enhance immune function. It can be used to:
- Containing renal carcinoma & cancer from spreading to other areas in the body
- Slowing down or stopping the growth and development of existing cancer cells
- Helping our immune system function better and helping it destroy cancer cells
Stem Cell Treatment for Kidney Cancer
Most patients diagnosed with Renal cell carcinoma (RCC) are treated with combinations of radiation therapy, chemotherapy, or surgery. Radiation-based therapies are disadvantageous as the high-energy particle rays do not target the cancer cells and destroy healthy cells, causing severe side effects. The levels of radiation exposure in chemotherapeutic doses must be limited to avoid organ toxicity. Therefore, RCC staging (TNM system)- qualified therapies require more precisely targeted treatments capable of killing cancer cells while sparing healthy cells.
Combining modern immunotherapies with UC-MSC+ stem cells employs a more holistic approach. It is significantly less toxic while yielding results that are similar to, and often superior to, those obtained with conventional therapies, depending on the type, age, and stage of diagnosis. Treatment of RCC and immune-boosting therapies are also more effective in achieving long-term tumor immunosurveillance while reducing the chance of relapse.
It is time to change how the world treats cancer.
Immunological therapies for kidney cancer can increase long-term disease-free survival and are prescribed as adjuvant therapy for patients with low white blood cell counts. Stem cell therapy for renal cancer (renal carcinoma) enhances the patient’s immune response by administering a naturally produced growth factor to increase the cancer-fighting capacity.[5]
Immunotherapy for kidney cancer has become a viable standard-of-care treatment and, in some cases, a complete cure. Immunotherapies manipulate or mobilize the patient’s immune system to treat or cure kidney cancer. Immunological therapies can also be performed via manipulation of genes using Dendritic cells (DCs), Immune modulators, monoclonal antibody therapy, adoptive cell transfer, and the new oncolytic virus therapy, which is a virus-based delivery system of modified genes where the payload uses the viruses as a host to carry past the patient’s immune system.
Modified CAR-T Cells for Kidney Cancer

Patients who are diagnosed with stage 3 kidney cancer who initially might have responded well to medications that target PD-1 protein (checkpoint inhibitors) can, over a short time, develop resistance to these therapies, especially if cancer has metastasized from its primary location to spawn additional kidney lesions and tumors. In such cases, CAR T Cells and genes encoded with tumor-associated antigens (TAA) induce an adequate response from the immune system.
Earlier clinical trials on late-stage kidney cancer focused on identifying the proliferating progenitor cells (CD34+) in human blood. These progenitor cells are stimulated by cytokines (GM-CSF and TNF-alpha) to differentiate rapidly into dendritic cells. In some cases, combining IL-4 and GM-CSF significantly increases the production of cancer-fighting dendritic cells from monocytes and macrophages.
Immunological therapy for kidney cancer might soon be the gold standard in the treatment of renal tumors for these reasons:
- Targeted Kidney cancer immunotherapy can target and debulk the tumor mass at the same time, kill the cancer via inducing a normal cellular response, and paracrine cell signaling
- Combining stem cells and immunotherapy growth factors helps reduce nearby lesions. It prevents metastatic formation at the cellular level, thereby improving cytoreduction while avoiding the destruction of normal cells.
- Renal Cancer stem cell therapies are non-toxic and may not require the use of chemotherapy and its adverse side effects.
- Immunological therapies help preserve memory responses (immunosurveillance), thereby significantly reducing the risk of relapse.
- Recent research indicates that adoptive CAR T-cell therapy is effective in treating renal cancer. This breakthrough therapy for kidney cancer is essential, as without the treatment, the estimated five-year survival rate is just below 8%.
Renal Cancer: Alternative Treatments
The Regeneration Center offers an alternative treatment for kidney cancer that can treat or reverse symptoms depending on the patient’s stage. The best defense from any cancer is first being informed about the disease to make an informed decision about biological treatment for cancer using stem cells.
Because kidney cancer biology varies widely from slow-growing localized tumors to aggressive metastatic disease, any discussion of “alternative” approaches has to start with clarity on what is realistically achievable: tumor control, symptom control, treatment tolerance, and quality of life are not the same endpoints. In evidence-based oncology, the core treatments for renal cancer remain surgery when feasible, targeted therapy, and immunotherapy, with radiation used in selected situations for symptom relief or local control. Many patients who look for complementary options are actually trying to solve practical problems that conventional care doesn’t always address well enough: fatigue, appetite loss, sleep disruption, anxiety, pain, weight loss, reduced physical conditioning, and the inflammatory “wear and tear” that can come with both the disease and its treatments.
If a clinic is discussing biologic or regenerative strategies, it is essential to distinguish between supportive regenerative care (focused on recovery and function) and direct anticancer therapy (focused on shrinking or eliminating tumors). At present, stem cell therapy is not an established, guideline-supported treatment for kidney cancer, and any claim that stem cells can treat cancer should be approached with caution unless it is offered within a regulated clinical trial framework with clear protocols, safety monitoring, and transparent endpoints. In some contexts, cell-based products can carry risks, particularly for cancer patients, including infection, immune complications, clotting events, and the theoretical concern of influencing tumor-supportive pathways in the wrong setting. That’s why reputable programs will emphasize coordination with the patient’s oncology team, a full review of staging and pathology, and a careful risk–benefit discussion rather than positioning cells as a replacement for standard-of-care cancer therapy.
A responsible “integrative” plan typically focuses on measurable, patient-centered goals: maintaining lean muscle and strength, optimizing nutrition and micronutrient status, managing inflammation safely, improving sleep and stress physiology, reducing fall risk, controlling pain, and monitoring kidney function closely (especially if one kidney has been removed or if targeted therapies affect blood pressure or renal perfusion). For patients seeking access to novel therapies, clinical trials in their home countries are often the most credible pathway because they do not require travel to Thailand for an extended period of time, and can provide defined inclusion criteria and objective outcome tracking. Ultimately, being informed means not only understanding the disease but also distinguishing between therapies proven to improve survival and those that are experimental or supportive, so patients can make decisions that are both hopeful and realistic.
Stem Cell Therapy for Kidney Cancer
Our stem cell therapy for kidney cancer is explicitly customized to the patient’s needs. The individualized protocol helps patients fight cancer using traditional cancer treatment and alternative natural cellular-based therapies. For nearly two decades, our approach to integrated healthcare has relied on research-based treatment plans that are comprehensive and tailored to patients’ medical needs to maximize the likelihood of success. The Regeneration Center offers a holistic approach to modern healthcare. We strive to combat cancer and alleviate underlying symptoms that can improve patients’ quality of life. Cancer stem cell treatment plans also help patients achieve long-term remission rates by addressing the disease’s root cause rather than its symptoms.
Warning and Dangers of Cancer Herbal Therapies
Some herbal-based treatments might help treat some symptoms associated with kidney cancer. However, patients diagnosed with cancer need to be extra cautious before consuming an herbal remedy from unknown sources. A compromised renal system may have greater difficulty metabolizing substances. Since many herbal preparations and extracts are alcohol-based, kidney cancer patients should always double-check all the ingredients before taking any herbs. Furthermore, some herbal supplements for kidney cancer can cause excessive bleeding and prevent blood from clotting properly.
Primary kidney cancer can be defeated. Our goal is to treat the body from the inside out and help patients achieve the most prolonged possible remission. Our natural cell-based approach to healthcare means we will work with you and your primary care doctor to determine the best overall treatment options. Our treatment evaluation for kidney cancer does require a review of current medical records. For patients who, for some reason, are not responding to traditional treatments or for whom surgery is not a good option, our team can review your Radiology scans (CT, ultrasound, or MRI) and laboratory tests to better target the tumor(s) and destroy them using minimally invasive techniques. We provide access to innovative kidney cancer treatment techniques and immunotherapies when appropriate. The Regeneration Center also offers its patients comprehensive follow-up care and survivorship programs ( In Thailand only) for patients recovering from kidney cancer.
The outlook for patients diagnosed with renal cancer has never been better. Thanks to modern medicine, many people survive the disease. The Regeneration Cancer Center has cared for patients worldwide who were diagnosed with different types of kidney lesions and stages of kidney cancer. Please contact us today to learn more about our treatment protocols and biological therapy for kidney cancer.
Published Clinical Citations
[1] ^ Linehan WM, Schmidt LS, Crooks DR, Wei D, Srinivasan R, Lang M, Ricketts CJ. The Metabolic Basis of Kidney Cancer. Cancer Discov. 2019 Aug;9(8):1006-1021. doi: 10.1158/2159-8290.CD-18-1354. Epub 2019 May 14. PMID: 31088840.
[2] ^ Turajlic S, Swanton C, Boshoff C. Kidney cancer: The next decade. J Exp Med. 2018 Oct 1;215(10):2477-2479. doi: 10.1084/jem.20181617. Epub 2018 Sep 14. PMID: 30217855; PMCID: PMC6170181
[3] ^Dziedzic K, Pleniceanu O, Dekel B. Kidney stem cells in development, regeneration and cancer. Semin Cell Dev Biol. 2014 Dec;36:57-65. doi: 10.1016/j.semcdb.2014.08.003. Epub 2014 Aug 13. PMID: 25128731.
[4] ^Bi LK, Zhou N, Liu C, Lu FD, Lin TX, Xuan XJ, Jiang C, Han JL, Huang H, Zhang CX, Dong W, Liu H, Huang J, Xu KW. Kidney cancer cells secrete IL-8 to activate Akt and promote the migration of mesenchymal stem cells. Urol Oncol. 2014 Jul;32(5):607-12. doi: 10.1016/j.urolonc.2013.10.018. Epub 2014 Jan 10. PMID: 24412633.
[5] ^ Fang P, Zhou L, Lim LY, Fu H, Yuan ZX, Lin J. Targeting Strategies for Renal Cancer Stem Cell Therapy. Curr Pharm Des. 2020;26(17):1964-1978. doi: 10.2174/1381612826666200318153106. PMID: 32188377