
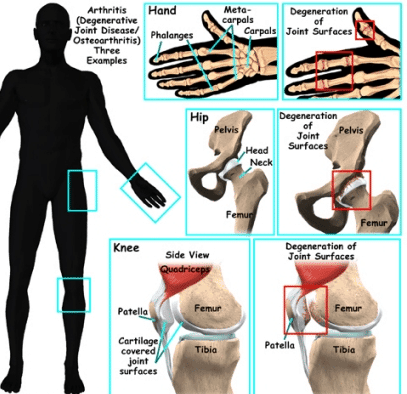
Arthritis comprises more than 128 distinct conditions and autoimmune diseases that can cause severe joint inflammation and pain. Stem cell transplantation for arthritis can help manage and permanently eliminate the arthritic condition, safely and effectively, using enhanced UC-MSC+ stem cells.
Arthritis is not a single condition; it is a family of more than 100 conditions that involve joint disease or joint pain. The two common forms of arthritis are osteoarthritis and rheumatoid arthritis. The disease affects people of all genders, ages, and racial backgrounds and is considered one of the leading causes of disabilities in the world. A diagnosis of arthritis can occur with age.
Common symptoms of arthritis include:
- Severe Pain in joints
- Swelling of joints
- Stiffness or decreased range of motion
- Redness
Rheumatoid Arthritis Vs. Osteoarthritis Treatment
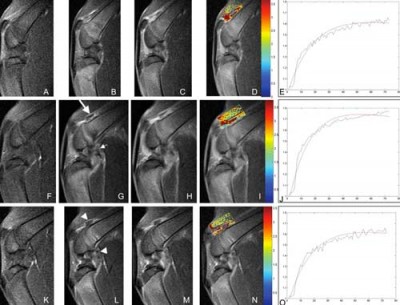
Signs often come and go, ranging from mild to moderate to even severe. Patients frequently ignore the symptoms for years but usually find that the disease degenerates even further over time, causing severe chronic pain and the inability to do typical day-to-day activities such as walking, climbing stairs, or exercising. If left untreated, Arthritis will cause permanent and visible joint damage, such as knobby/knotted finger joints. An MRI or X-ray is needed to thoroughly evaluate treatment options in individuals without symptoms. Some types of severe arthritis can also affect the patient’s heart function, vision, impaired kidney function, skin, lungs, and circulatory system.
Risk factors for acquiring a Diagnosis of Arthritis include:
- Genetics or Family history: Arthritis can run in families, so patients with parents or siblings with the disorder are at increased risk of developing the disorder. Genes can also increase susceptibility to environmental factors that trigger the onset of arthritis. Testing for genetic arthritis is now available.
- Gender – Women are much more likely to develop rheumatoid arthritis than men, while most patients who get diagnosed with gout ( another type of arthritis) are men.
- Patients with a previous joint injury – People who have injured and surgically treated hip or knee joints are at a much higher risk of developing arthritis in that joint. An alternative to knee surgery or reducing the risk of knee osteoarthritis, is hip Surgery, or shoulder surgery
- Obesity/Body Weight—Excess weight can damage joints and put extra stress on joints such as knees, spine (spinal stenosis), or hips. Therefore, overweight people have a much higher risk of developing arthritis as they age.
- Age: The risk of acquiring many types of arthritis increases with age.
There are numerous well-known types of joint arthritis. The two main types of joint arthritis are osteoarthritis and Rheumatoid Arthritis. RA, or Rheumatoid joint inflammation, is a constant ailment. RA typically begins with irritation, fatigue, joint discomfort, and/or stiffness. As this problem worsens, you will experience frequent flu-like symptoms and muscle pains. Osteoarthritis, on the other hand, is a “wear & tear” problem. Osteoarthritis is more common with age and is now manageable with Stem Cell treatment for Osteoarthritis. Osteoarthritis begins with stiffness and joint discomfort and is treatable with stem cell treatment for osteoarthritis.
Ankylosing Spondylitis & Spinal Arthritis
UC-MSC+ Stem Cells for Autoimmune Arthritis
Additional types of joint inflammations that are treatable in a short trip to Thailand include:
- Stem Cell Treatment for Lupus

- Cell Transplants for Fibromyalgia
- Stem cell therapy for Gout
- Therapy for Septic Arthritis
- Stem Cell Treatment for Sarcopenia
- Stem Cell Treatment for Rheumatoid Arthritis
- Stem Cells for Hip Arthritis
- Treatment for Psoriatic Joint Inflammation
- Stem Cell Treatment for the Knee
- Treating Arthritis in the Wrist and Hands
- Stem Cell Therapy for Shoulder Arthritis
The types of stem cells needed for treatment depend on the autoinflammatory vs autoimmune disease the patient is diagnosed with. However, (UC-MSC+) mesenchymal stem cells offer a viable alternative to invasive knee replacement surgery or hip replacement surgery. The Regeneration Center provides a safe and effective cell-based treatment for degenerative Arthritis that can quickly help relieve pain, problems, and unnecessary physical suffering. Most adults aged 40-65 develop cartilage and joint degeneration that leads to osteoarthritis. These conditions can safely be treated today using UC-MSC+ Cells for Joint inflammation and Arthritis.
Stem cell therapy for cartilage regeneration
Cell regenerative medicine allows the replacement cells to travel throughout your body through a process known as “homing.” Homing means the cell is actively “homing” to distressed/injured areas throughout your body.[1] Autologous regeneration of joints requires harvesting the cells from autologous fat, peripheral blood, or marrow, then separating and expanding the mesenchymal cells over 2-4 weeks. [2] For older patients or those with an underlying medical condition that will not allow us to take stem mesenchymal stem cells from their body (bone marrow-derived), we can offer isolated allogeneic stem cells to begin the tissue repair process in the cartilage matrix.

Mesenchymal Stem Cell Therapy for Cartilage Regeneration
Some background information is needed to evaluate the long-term safety and efficacy of mesenchymal stem cell (UC-MSC) treatments for osteoarthritis (OA). UC-MSC cells can be easily obtained in several areas, including bone marrow, peripheral blood, cord tissue, placental tissue, and Wharton’s jelly. When properly extracted, they are considered safe and do not prevent future treatments if needed. The isolated UC-MSC stem cells are cultured for 7-10 days at our stem cell lab in Bangkok before they are injected back into the joints affected by OA. This process can begin before patient arrival, allowing treatment to begin on Day 1.
Stem Cell Delivery Methods
For patients with moderate multi-level disc degeneration, multiple sessions of clinical grade expanded UC-MSC+ Mesenchymal Cells will be used along with our proprietary mix of growth factors that can include Transforming Growth Factor-beta (TGF-β), Fibroblast Growth Factors (FGF), Platelet-Derived Growth Factors (PDGF), Bone Morphogenetic Proteins (BMPs), Insulin-like Growth Factor-1 (IGF-1), Vascular Endothelial Growth Factors (VEGF), Connective Tissue Growth Factors (CTGF), Epidermal Growth Factors (EGF), and Nerve Growth Factors (NGF). Isolated cells and growth factors are delivered via intravenous infusion, direct local injection, intradiscal injection, intrathecal injection, fluoroscopy-guided stem cell delivery (in a hospital setting only), or a combination of these methods to achieve optimal results.
What are the disadvantages of using stem cells to treat Arthritis?
There are several different methods for using isolated MSC+ cells in treatment. One way involves expanding the undifferentiated stem cells in our stem cell lab to create a more uniform population of cell types needed before introducing them back to the patient over two weeks. This approach allows us precise control over the types and quantities of cells used. An alternative and less effective way is to use bone marrow aspirate concentrate (BMAC) or stromal vascular fraction (SVF) cells. This method generally does not use extensive cell manipulation and has a more straightforward regulatory pathway. However, the lack of cell culturing offers fewer MSC cells compared to expanded protocols (UC-MSC+)cells. In addition to bone marrow and adipose tissue, other sources of UC-MSC cells include isolating cells from amniotic fluid and cord membranes. Allogeneic MSC cells from these sources can be used since they have low immunogenicity and can avoid immune responses in recipients. This approach is often more beneficial for older patients or those with multiple co-morbidities whose UC-MSC cells may have reduced regenerative potential for knee OA and require total knee replacement surgery or several rounds of intra-articular injection of mesenchymal stem cells and osteoarthritis therapy.
What is the success rate of stem cell treatment for osteoarthritis?
UC-MSCs primarily refer to stromal cell populations expanded ex vivo. For over 40 years, UC-MSC cells have been used in musculoskeletal treatments because of their ability to become tissue-specific cells like osteoblasts, chondrocytes, and tenocytes. However, about a decade ago, the Regeneration Center began isolating MSC cells to enhance their ability to sense their environment and release bioactive molecules, such as cytokines, antioxidants, and trophic growth factors. These molecules and growth factors are used with UC-MSC+ stem cells to re-establish tissue balance after an injury. Thus, our combination protocol using UC-MSC+ cells yields significantly higher success rates by incorporating medicinal signaling cells and tissue-specific growth factors. Clinical trials have shown that expanded UC-MSC cells can help repair tissues by reducing inflammation, limiting stress response, and recruiting immune and reparative cells. Regenerative medicine research has also shown that a pro-inflammatory environment can trigger the anti-inflammatory effects of UC-MSC+ cells. For example, UC-UC-MSCs exposed to synovial fluid or inflammatory cytokines show increased anti-inflammatory molecule production and inhibit T-cell proliferation. Learn about the Top 10 foods to fight osteoarthritis. While our findings don’t negate the idea that UC-MSCs can directly differentiate into tissue-specific cells, it’s difficult to achieve good results from a small sample of UC-MSC from bone marrow aspirate concentrate (BMAC) or stromal vascular fraction (SVF) injected into a joint over a short 1-3 day protocol, which can reach multiple damaged areas and produce new cartilage. Therefore, our treatment protocol is unique as it uses two mechanisms of UC-MSC action (paracrine and direct cell differentiation), which are not mutually exclusive. Still, their differences are crucial for understanding and setting realistic expectations for patients undergoing stem cell therapy for Arthritis.
Can stem cells reverse osteoarthritis?
Many studies have assessed the efficacy of regenerative treatments for osteoarthritis (OA), but there are limitations to what is realistically feasible. When treating patients with OA, they should expect rapid symptom relief due to UC-MSC+ cells’ ability to release various molecules that promote tissue repair and reduce inflammation. However, if one lacks tissue-specific growth factors, the duration of these effects will be limited. For a more permanent solution for OA and femoral neuropathy, a protocol should employ multiple cell types, growth factors, and delivery methods, followed by appropriate rehabilitation to ensure sustained long-term benefits of stem cell therapy. Our treatment goal is to improve a patient’s quality of life for longer than one year. Still, it requires several steps to be completed to achieve satisfactory results, especially for those who have been suffering for a long time and have been using daily painkillers or anti-inflammatory drugs with known side effects. Predicting a patient’s response to the Regeneration Center treatment for Arthritis can be complex without reviewing the patient’s medical information, as each person’s symptoms, stages, and severities vary.
TREATMENT RISKS & PRECAUTIONS
Please note that not all patients are suitable candidates for stem cell therapy for Osteoarthritis or Gouty Arthritis. Patients with advanced joint damage, severe deformities, multiple joint involvement, or other significant health issues may not be good candidates for treatment.Expanded UC-MSC+ Stem Cells for Osteoarthritis
Stem cell research for arthritis has enabled us to develop a protocol focused on safety and efficacy. Our stem cell treatments for arthritis combine an affordable method of managing arthritic degenerative conditions that can assist your body in healing faster, reducing pain and stiffness, and improving function. The protocol for treating Arthritis Is in 2 phases, using Mesenchymal Cells combined with growth factors to increase the percentage of blood platelets. Cellular therapy for arthritis combines osteogenic cartilage cells & growth factors to expedite recovery in damaged tissues and knee cartilage. Stem cell research has shown that UC-MSC cells are the gold standard alternative therapy for tissue repair, via essential anti-inflammatory elements and growth factors that support cell homing and instruct the body’s cells to initiate the natural healing process.
Stem Cell Therapy for Osteoarthritis
Isolated and enhanced UC-MSC+ stem cells are introduced to multiple points near the joints or tissue bordering the troublesome areas. [3] Using only the latest techniques to treat arthritis, these repair stem cells modify and repair damaged tissues and instruct damaged cells to self-repair, resulting in pain relief.[4] We are the leading treatment provider center of Allogeneic Hematopoietic Mesenchymal and Autologous Stem Cell Therapy from adipose tissue, and peripheral blood, bone, & Stem cell treatment for Rheumatoid Arthritis. Other cell-based therapies we offer include treatment of spinal trauma, treatment for heart disease, peripheral neuropathy, treatment for diabetics, treatment for Autism, treatment of knee osteoarthritis, reduced knee pain, and stem cell treatment for kidney failure. [5]
Before and After Stem Cell Therapy for Arthritis

Avoid Joint Replacement Surgery With Stem Cell Therapy in the Knee
Total Number of Adult Stem Cell Injections: The total number of Endogenous Mesenchymal Stem cells, cartilage cells ,exosomes, and regenerative growth factors to repair tissue will vary based on patient needs, locations of knee pain, and severity of cartilage defects. Eligibility criteria depend on the required injury; treatment can be administered via guided radiography, intravenous infusion, Direct injection, intra-articular injection, or intrathecal administration of different cell types.[6]
Rehabilitation Post-Treatment: Physical Rehabilitation and weight-loss programs are optional but strongly recommended. Complete physical rehabilitation services following regenerative therapy can be provided upon request, for 2-3 hours per day, up to 5 days per week.
The Total Time Required To Treat the Hip and Knee is estimated to be around two weeks (depending on the type and seriousness of the condition). Medical and travel visas for extended accommodations at a hotel or apartment for the patient and family can also be provided upon request.
Treating Osteoarthritis with Stem Cells
Cost of Stem Cell Treatment for Osteoarthritis in 2026
UC-MSC+ Stem Cell treatment for arthritis and osteoarthritis cell therapy will require an estimated 10-14 days. Due to the varying degrees of severity, our orthopedic team will need to evaluate potential patients to establish an appropriate protocol. Upon completion of the medical review, a detailed treatment plan will be provided, including the exact number of nights required and the total medical-related costs. To begin the evaluation process for our multi-stage arthritis treatment protocol with intra-articular injections, please prepare your recent medical records, such as radiology scans and blood tests, and contact us today.
Published Clinical Citations
[1] ^ Hauser, Ross A, and Amos Orlofsky. 2013. Regenerative injection therapy with whole bone marrow aspirate for degenerative joint disease: a case series. Clinical medicine insights. Arthritis and musculoskeletal disorders (September 4). doi:10.4137/CMAMD.S10951. https://www.ncbi.nlm.nih.gov/pubmed/24046512
[2] ^ Kheansaard, Wasinee, Sumana Mas-Oo-di, Surasak Nilganuwong, and Dalina I Tanyong. 2012. Interferon-gamma induced nitric oxide-mediated apoptosis of anemia of chronic disease in rheumatoid arthritis. Rheumatology international, no. 1 (January 19). doi:10.1007/s00296-011-2307-y. https://www.ncbi.nlm.nih.gov/pubmed/22258456
[3] ^ Oshita, Koichi, Kunihiro Yamaoka, and Yoshiya Tanaka. 2013. [Regulation of osteoclastogenesis by human mesenchymal stem cells leading to application of a novel treatment for rheumatoid arthritis]. Journal of UOEH, no. 1 ( 1). https://www.ncbi.nlm.nih.gov/pubmed/23475022
[4] ^ Roelofs, A J, J P J Rocke, and C De Bari. 2013. Cell-based approaches to joint surface repair: a research perspective. Osteoarthritis and cartilage, no. 7 (April 15). doi:10.1016/j.joca.2013.04.008. https://www.ncbi.nlm.nih.gov/pubmed/23598176
[5] ^ Turajane, Thana, Ukrit Chaweewannakorn, Viroj Larbpaiboonpong, Jongjate Aojanepong, Thakoon Thitiset, Sittisak Honsawek, Juthatip Fongsarun, and Konstantinos I Papadopoulos. 2013. Combination of intra-articular autologous activated peripheral blood adult stem cells with growth factor addition/ preservation and hyaluronic acid in conjunction with arthroscopic microdrilling mesenchymal cell stimulation Improves quality of life and regenerates articular cartilage in early osteoarthritic knee disease. Journal of the Medical Association of Thailand = Chotmaihet thangphaet, no. 5. https://www.ncbi.nlm.nih.gov/pubmed/23745314
[6] ^ Zhen, Gehua, Chunyi Wen, Xiaofeng Jia, Yu Li, Janet L Crane, Simon C Mears, Frederic B Askin, et al. 2013. Inhibition of TGF-β signaling in mesenchymal stem cells of subchondral bone attenuates osteoarthritis. Nature medicine, no. 6 (May 19). doi:10.1038/nm.3143. https://www.ncbi.nlm.nih.gov/pubmed/23685840