

Connective tissues in the human body are structural components that hold the body’s cells together. These tissues form a matrix (framework) for the body and are composed of two major structural protein molecules: elastin and collagen. Several types of collagen protein vary in quantity depending on the tissue in which they are found. Elastin protein can stretch and return to its original length, like springs or a rubber band. Elastin is also a significant component of tissues that attach bones to other bones (ligaments) and of our skin. Patients with connective tissue disorders often exhibit elastin and collagen damage due to chronic inflammation.
What is connective tissue (CT) disease?
Connective tissue disorders are a group of medical conditions. A connective tissue disease (CT) diagnosis is made when the connective tissues in the body are the primary target of pathology. Patients with connective tissue diseases often show abnormal immune system function with significant inflammation in the tissues due to autoimmune attacks (the immune system attacks its body tissues) [1]
Any diseases in which collagen is weak or inflamed are called collagen diseases. For some patients, collagen vascular disease is diagnosed because the connective tissues are associated with abnormalities in blood vessels.
What causes connective tissue disorders?
For many patients, a diagnosis is considered idiopathic (unknown cause). For others, direct links to genetic factors can increase the risk of developing connective tissue disorders. For others, a diagnosis is likely due to a combination of environmental factors ( exposure to toxins) and genetic predispositions resulting in the development of connective tissue disorder.
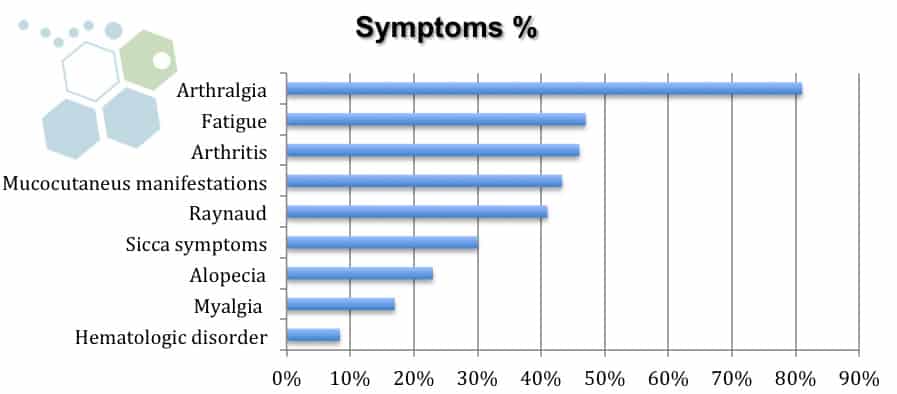
Signs and symptoms of connective tissue disease
A prevalent symptom of connective tissue disease is premature fatigue, which can sometimes be misdiagnosed as FMS or CFS. Other indicators of (mixed) connective tissue disease include:
- Fevers or the constant feeling of being unwell
- Chronic joint and muscle pain. Knee or hip joints become swollen, inflamed, or deformed, similar to patients with rheumatism.
- Raynaud’s phenomenon is when patients have cold /numb toes or fingers [2]
- Frequent Rash – Reddish or brown patches over the knuckles
- Swollen hands or fingers
Diagnosis of connective tissue diseases
Several tests can be done to identify particular types of connective tissue disease. This can be done via a simple physical examination but often requires several rounds of blood tests, radiology scans, and genetic screenings to get clinically diagnosed with connective tissue disease.
Genetic risk factors for developing connective tissue disorders
Several types of connective tissue diseases are caused directly by genetic (familial) inheritance, including:
- Marfan syndrome – Patients can have tissue abnormalities in the lungs, eyes, heart, aorta, and musculoskeletal system
- Ehlers-Danlos syndrome – Patients have very fragile & loose skin with hyperextensible joints
- Autosomal dominant Polycystic kidney disease
- Fibromuscular dysplasia
- Osteogenesis imperfecta type I [3]
- Menkes’ disease
Other connective tissue disorders cannot be regularly attributed to gene abnormalities (scleroderma & systemic lupus erythematosus). These connective tissue disorders can occur for unknown reasons, but may involve weaker gene factors that predispose them to develop the disease. This group is sometimes characterized by overactivity in the immune system, resulting in significant additional antibodies in the blood circulation. To learn more about our genetic screenings for autoimmune and connective tissue diseases, visit here.
Autoimmune diseases known to cause connective tissue disease
The cause of idiopathic connective tissue disease is not known. The Regeneration Center believes that the disorder can be triggered by environmental factors, especially among those who may already be genetically susceptible to some patients who are diagnosed with Type 1 Diabetes [4]. In such cases, the protective immune system malfunctions, producing specific antibodies that attack the body’s tissues.
These autoimmune connective tissue diseases can include:
- Hashimoto’s thyroiditis
- Degenerative Disc Disease
- Necrotizing vasculitides
- Pancreatitis
- Relapsing polychondritis
- Systemic lupus erythematosus – SLE
- Sporadic inclusion body myositis
- Multiple Sclerosis
- Scleroderm (overlap syndrome)
- Sjögren syndrome
- Osteoarthritis ( ubiquitous noninflammatory disease of the joints, particularly affecting the hips, shoulders, and knees )
- Osteoporosis
- Dermatomyositis & Autoimmune Inclusion Body Myositis
- Polymyositis
- Rheumatoid arthritis
- Rheumatic fever
- MG with no detectable AChR and MuSK antibodies
- Transverse Myelitis
- Thrombotic thrombocytopenic purpura
These autoimmune diseases are considered classical connective tissue disorders because they have a “classic” / typical presentation that most physicians can quickly recognize using tests & examinations. Each classic symptom also shows abnormalities in specific antibodies commonly detected in blood and pathology tests. However, it should be noted that the progression rates of each classic symptom vary from patient to patient, with some evolving very slowly or rapidly.
What is Overlap Syndrome?
For some patients in the early stages, the diagnosis is considered “undifferentiated” as CVD (collagen vascular disease) or UCTD (undifferentiated connective tissue disease) until additional symptoms appear. The transition from CVD to UCTD may occur over time or never materialize. In some cases, the undifferentiated features might disappear entirely, at which point the disease becomes detectable and resolves naturally. If a patient has more than one type of autoimmune connective tissue disease, the condition is often classified as overlap syndrome.[5]
What is Mixed Connective Tissue Disease (MCTD)?
One common overlap syndrome is shared by diseases such as lupus, scleroderma, and polymyositis; these are called MCTD (mixed connective tissue disease) & Sharp’s syndrome.
Traditional treatment options for Connective tissue disorder
Current medicinal treatment options for mixed connective tissue disease can help manage the signs and symptoms and are prescribed depending on the stage and severity of the diagnosis and the patient’s symptoms. Traditional medications for the disease can include:
- Calcium channel blockers, including Adalat CC, Procardia (nifedipine), and Norvasc (amlodipine), help relax the muscle walls of blood vessels and are often used in patients with Raynaud’s phenomenon
- Corticosteroid medications such as Deltasone or Rayos (prednisone) can help stop the immune system from attacking otherwise healthy cells and suppress inflammation. Some side effects of corticosteroids can include wild mood swings, high blood sugar, weight gain, weakened bones, increased blood pressure, and cataracts.
- Pulmonary hypertension medications such as Tracleer (Bosentan) or sildenafil (Viagra or Revatio)
- Antimalarial medications such as Plaquenil (Hydroxychloroquine) treat mild cases of mixed connective tissue disorders and can sometimes help prevent flare-ups.
- Other immunosuppressants may also be prescribed based on the patient’s symptoms and stage.
Stem Cell Treatment for Connective Tissue (CT) Disease
Compared to traditional medical treatments such as immunosuppressive medications and biologicals, UC-MSCs+ stem cell transplants for connective tissue diseases do not just suppress the patient’s immune system. Still, they can promote fundamental changes in the immune system, which are vital for long-lasting remission. Other benefits of stem cells for MCTD include:
- Stem cells can help create the environment for stem cells to home, cell signaling, and the development of new niches for cellular differentiation.
- Modified stem cells help with the depletion of B lymphocytes and autoaggressive T Cells (Induction of regulatory T cells)
- Multipotent mesenchymal stromal cells (UC-MSC+) can differentiate into cartilage, bone, and other connective tissues.
- UC-MSCs+ Stem cells offer a wide array of immunomodulatory effects, abrogating the inflammatory response and reducing autoantibodies.
- Stem cells can help restore the patient’s normal immune regulation.
- Modified stem cells can help reverse stromal cell abnormalities.
TREATMENT RISKS & PRECAUTIONS
Please note that patients with multiple comorbidities or immune system dysregulation may face travel limitations to Thailand. All potential candidates seeking therapy should be approved in advance based on basic medical records and recent blood panels, which may include markers of inflammation such as C-reactive protein and erythrocyte sedimentation rate (ESR). Depending on the stage and severity of the diagnosis, additional tests for antibodies (to detect autoimmune conditions) and imaging tests, such as an MRI or CT Scan, may be required. Please contact us for more information.The Regeneration center protocol combines isolated UC-MSC+ stem cells with several types of growth factors, including:
- Vascular endothelial growth factor (VEGF)
- Epidermal growth factors
- Hepatocyte growth factor
- Insulin-like growth factors
- Stromal cell-derived factor-1
- Fibroblast growth factors
Our proprietary stem cell treatment for Connective Tissue Diseases & mixed connective tissue diseases requires 10-14 days in total, and helps in restoring cytokine imbalances, inducing angiogenesis, modulating the immune system, and promoting the reparative effects of UC-MSC+ stem cell transplants.
The developmental mechanisms of osteogenesis
The human joints are discrete organs of various connective tissues, including tendons, cartilage, bone, ligaments, and muscles. Any trauma or degeneration in these tissues can cause joint dysfunction, which leads to restricted function and movement. In the past, this meant having risky, common surgeries. Recent studies have shown that nearly 45% of all adults live with some joint-related condition. This number is almost the same as those diagnosed with type 2 diabetes, heart disease, heart attacks, heart failure, COPD (chronic respiratory diseases), or pulmonary fibrosis combined.
In orthopedics, the demand for minimally invasive stem cell therapies is also driven by the lack of adequate alternative treatments for common connective tissue degenerative diseases such as spinal arthritis. Several progenitor and self-renewable stem cell types can be differentiated into multiple musculoskeletal cell lineages. Due to rapid advancements in molecular biology and stem cell science, regenerative therapies have emerged as effective treatments for existing joint-relevant connective tissue diseases. They can help preserve healthy joints for years to come.
To treat immune-mediated inflammatory disease, The Regeneration Center has developed a unique combination therapy using isolated UC-MSC+ stem cells and tissue-specific growth factors that are particularly effective in stabilizing an otherwise abnormal rate of osteogenic differentiation. UC-MSC+ cells are engineered to provide low immunogenicity and immunomodulatory properties. UC-MSCs+ therapy for connective tissue disorders does not require immunosuppressive medications. The UC-MSC+ cells used can be autologous or allogeneic. Allogeneic UC-MSC+ cells do not express HLA-DR, making them ideal therapeutic candidates for transplantation in patients with immune-mediated disorders. UC-MSC+ can eradicate dysfunctional cells and restore immune system homeostasis by replacing damaged cells with differentiated B and T cells.
The Regeneration Center Difference
Total Number of UC-MSC+ Cell Infusions: Total Endogenous Cell Count, UC-MSC+ Cell count, and tissue-specific growth factors will vary based on patient symptoms.
Types of Injections for Treating SLE: UC-MSC+ Mesenchymal Stem Cells. Depending on the severity of the patient’s needs, treatment injections will be made via Intravenous Drip, Intra-Articular Injections, Subcutaneous Injections, Intramuscular Injections, Intrathecal injections, or a combination of methods using multiple delivery routes. Patients with various conditions may require cell delivery via a CT-guided scope (Hospital Setting Only)
Rehabilitation Post Treatment: Physical Rehabilitation in Bangkok is optional but highly recommended. Post-therapy physical rehab services can be provided upon request for 2-3 hours per day, up to 5 days per week.
Total Treatment Time Required: It is estimated to be approximately 2 weeks (depending on the type and severity of the condition). Medical and travel visas for extended accommodations at a hotel or apartment for the patient and family can also be provided upon request.
Connective Tissue Disease Treatment Guidelines for 2026
The cost of treating dense regular connective tissue, collagen vascular disease, and overlap syndrome will vary depending on the degree of severity. Our medical team will need to evaluate the patients using the current medical records. Evaluations can be done in person or online (submitting documents online). After review, a detailed treatment plan will be provided, including specifics such as the total number of nights required and the total medical costs for stem cell treatment of connective tissue disease. Please prepare all current medical records and contact us today to begin the evaluation process.
Published Clinical Citations
[1] ^Peng, Hairong, and Johnny Huard. “Stem cells in the treatment of muscle and connective tissue diseases.” Current opinion in pharmacology vol. 3,3 (2003): 329-33. doi:10.1016/s1471-4892(03)00051-1 https://www.ncbi.nlm.nih.gov/pubmed/12810201
[2] ^ Usas, Arvydas, and Johnny Huard. “Muscle-derived stem cells for tissue engineering and regenerative therapy.” Biomaterials vol. 28,36 (2007): 5401-6. doi:10.1016/j.biomaterials.2007.09.008 https://www.ncbi.nlm.nih.gov/pubmed/17915311
[3] ^Seong, Jeong Min et al. “Stem cells in bone tissue engineering.” Biomedical materials (Bristol, England) vol. 5,6 (2010): 062001. doi:10.1088/1748-6041/5/6/062001 https://www.ncbi.nlm.nih.gov/pubmed/20924139
[4] ^Zha, Kangkang et al. “Recent Advances in Enhancement Strategies for Osteogenic Differentiation of Mesenchymal Stem Cells in Bone Tissue Engineering.” Frontiers in cell and developmental biology vol. 10 824812. 23 Feb. 2022, doi:10.3389/fcell.2022.824812 https://www.ncbi.nlm.nih.gov/pubmed/35281084
[5] ^ Derakhshan, Tahereh et al. “Human Mast Cell Development from Hematopoietic Stem Cells in a Connective Tissue-Equivalent Model.” Tissue engineering. Part A vol. 25,21-22 (2019): 1564-1574. doi:10.1089/ten.TEA.2018.0347 https://www.ncbi.nlm.nih.gov/pubmed/30896346