
SpA (Spondyloarthropathies) disorders are a family of autoimmune inflammatory conditions that share common manifestations, such as inflammation of the sacroiliac joints, the spine, and peripheral joints, and are often associated with genetic factors, such as the HLA-B27 gene. Members of the spondyloarthropathy family include reactive arthritis, axial spondyloarthritis (axSpA), psoriatic arthritis, and arthritic spondylitis, which are also associated with inflammatory bowel diseases such as ulcerative colitis & Crohn’s disease.
Ankylosing Spondylitis & Spinal Arthritis
What is ankylosing spondylitis?
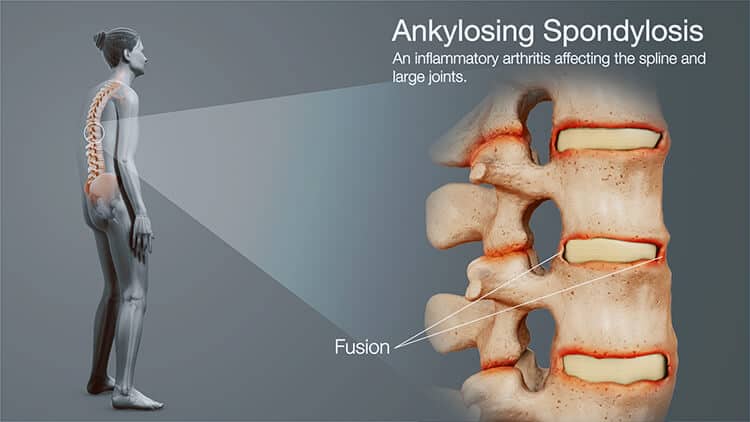
Ankylosing spondylitis (AS) is a progressive inflammatory rheumatic disease primarily found in the axial skeleton and sacroiliac joints.[1] The primary clinical manifestation of AS is frequent back pain and progressive stiffness in the “Bamboo spine.” Other affected areas include Oligoarthritis (arthritis affecting two to four joints), usually in the shoulders and hips. Other patients report degenerative disc disease, enthesopathy (a disorder of the connective tissues between bones and tendons [entheses]), ligament enthesopathy, and anterior uveitis. Although extensive research has been conducted, our current understanding of the pathogenesis of ankylosing spondylitis remains limited. Common causes are usually attributed to hereditary reasons (e.g., HLA-b27), infections, and autoimmune attacks.
Ankylosing spondylitis is a type of arthritis that affects the spine and causes severe inflammation of the spinal joints, leading to chronic pain and frequent discomfort. In patients with more advanced AS, chronic inflammation leads to new bone formation, causing segments of the spinal cord to fuse (fixed, immobile position) and is commonly referred to as a bamboo spine. Bamboo spine generally develops due to ossification in the outer fibers of the annulus fibrosus of the intervertebral discs, leading to Osteonecrosis of the hip or the formation of syndesmophytes (bony growth originating inside a ligament) between the adjoining vertebrae.
Spondyloarthropathy is highly heritable and is often associated with progressive rigidity, rheumatoid arthritis, peripheral arthritis, gouty arthritis, and chronic inflammatory responses in the spine and pelvis.
Who Gets Ankylosing Spondylitis?
Who Gets Ankylosing Spondylitis?
For many patients, ankylosing spondylitis (AS) is diagnosed relatively early in life—often in the late teens through the 30s because symptoms typically begin years before clear imaging changes appear. The classic pattern is inflammatory back pain and stiffness that improve with movement, along with reduced spinal mobility over time. As the condition progresses, this can translate into measurable physical limitations, work impairment, and a real decline in day-to-day quality of life. Family history matters: having a first-degree relative with AS or related “spondyloarthritis” conditions raises risk, reflecting the strong genetic contribution to disease susceptibility.
Genetics is a major piece of the picture, and HLA-B27 is the best-known marker. More than 90% of patients in many (especially Northern European) cohorts carry HLA-B27, although this percentage varies by ancestry and geography. Most HLA-B27–positive individuals never develop AS; therefore, it is a risk factor, not a diagnostic criterion in itself. Beyond HLA-B27, other immune-related genes are implicated (for example, pathways involved in antigen processing and mucosal immunity), which helps explain why AS can cluster with intestinal inflammation. Clinically, AS also overlaps with related disorders such as inflammatory bowel disease, psoriasis, and reactive arthritis, and patients may present with features like uveitis (eye inflammation), enthesitis (tendon/ligament insertion pain), or peripheral joint symptoms rather than “textbook” low-back complaints.
Epidemiologically, men are still diagnosed about 2–3 times more often than women, but part of that gap is thought to reflect differences in presentation and diagnostic delay: women may have less obvious radiographic sacroiliitis early on, more widespread pain, or more peripheral symptoms that can be misclassified for longer. On the immunology side, AS is tightly linked to inflammatory signaling networks, particularly TNF-α and the IL-17/IL-23 axis, which is consistent with the effectiveness of biologic therapies targeting these pathways in many patients. Markers like ANCA have been reported in small subsets or in overlap contexts, but they are not considered a core biomarker for AS and don’t reliably track with severity; when ANCA is positive, it usually prompts clinicians to think carefully about alternative or additional inflammatory diagnoses rather than using it as a staging tool for AS.
Symptoms & Complications of Axial Spondyloarthritis
As Ankylosing spondylitis progresses, patients report chronic spinal inflammation, and radiographic imaging often shows new bone formation across all spinal segments. Eventually, calcification of vertebral and paravertebral ligaments will aggravate nerve endings, resulting in chronic pain. The rate of new bone formation varies from patient to patient but is generally attributable to increased differentiation of osteoblast cells. Patients diagnosed with spinal arthritis are at very high risk of developing spinal fractures, osteoporosis, lupus, spinal cord injuries, hypertension, heart diseases such as CHF, pulmonary complications leading to COPD or IPF (upper portion of the lung), and metabolic syndromes such as sarcopenia, type 1 diabetes, type 2 diabetes, neuropathy, femoral nerve pain and diabetic nephropathy. Patients with AS also have a higher prevalence of dementia and Alzheimer’s, primary Sjogren’s Syndrome, ALS, and MND compared with the general public. If left untreated, the condition degenerates over time, resulting in spinal mobility loss and limitations in lateral and anterior flexion movement. Other systemic failures common for patients with AS include weight loss, chronic fatigue, and fever. Pain is often worse with rest for most patients but can improve with light physical activity. [2]
Diagnosing Ankylosing Spondylitis Stage 4 Advanced
Ankylosing spondylitis and axial spondyloarthritis can be diagnosed today by assessing changes in the sacroiliac joints and spine using imaging modalities such as MRI. Genetic screenings are also done to check for the presence of the HLA-B27 marker. Patients who are HLA-B27 positive have a better-than-average risk of developing certain types of autoimmune disorders. For patients with acute inflammatory attacks, simple blood tests can measure the concentration of CRP (C-reactive protein) and ESR 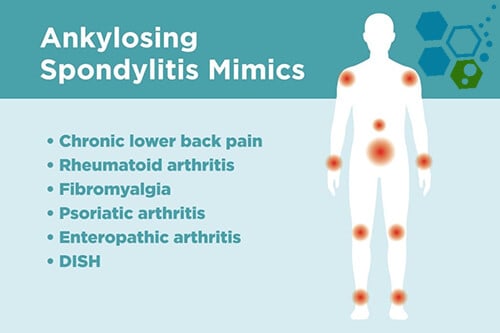 (erythrocyte sedimentation rate). However, it should be noted that many patients with ankylosing spondylitis have normal ESR & CRP levels, so normal ESR and CRP results do not necessarily reflect the degree of inflammation.
(erythrocyte sedimentation rate). However, it should be noted that many patients with ankylosing spondylitis have normal ESR & CRP levels, so normal ESR and CRP results do not necessarily reflect the degree of inflammation.
These general criteria for diagnosing spondyloarthritis include:
- Frequent inflammatory back pain
- Family history of inflammation in the tendon-bone attachments, heel, shoulder, or hip joints
- Positive test for HLA-B27 Gene – DNA Testing at Regen Center
- Elevated levels of inflammation measured by CRP/hs-CRP or ESR Blood tests
- Family history of spondyloarthritis or other rheumatic/autoimmune conditions
- Previous diagnosis of chronic lymphocytic thyroiditis
- A fair response to nonsteroidal anti-inflammatory drugs (NSAIDs)
- Psoriasis
- History of spinal inflammation
- Inflammatory bowel disease
- Frequent inflammation of the eye (uveitis)
- Inflammation of the sacroiliac joint was confirmed with an MRI scan
Treatment options for Ankylosing Spondylitis in 2026
Traditional antirheumatic drugs can help improve back pain, disturbed sleep, and peripheral arthritis acute-phase responses, and can temporarily improve quality of life; however, the major contributing factor in axial spondyloarthritis is new bone formation, which is generally not affected. With this new alternative, AS treatment focuses on modulating osteogenic differentiation to prevent new bone formation and induce sustained disease remission.[3]
Traditional Treatments of Spondyloarthritis:
There is currently no cure for hereditary ankylosing spondylitis. The success of modern biological treatments and traditional pharmaceutical medications can help contain the disease and reduce pain; however, early intervention is vital. It can be challenging to obtain a definitive diagnosis early, necessitating a prolonged diagnostic process. Annual physical examinations and tests can be used to identify the underlying cause of symptoms.
Commonly used non-surgical treatments for Ankylosing spondylitis include Physical therapy & Exercise. Regular physical therapy can help restore some joint function. Occupational therapy is a great way to strengthen the tissues and muscles needed for a flexible, healthy body. Non-impact exercises can provide patients with fast relief of pain and stiffness. This natural therapy can help reduce the risk of future disabilities.
Prescription Medications – DMARDs – NSAIDs
NSAIDs (nonsteroidal anti-inflammatory drugs) are the most common first treatment used for controlling symptoms. The family of such medications includes naproxen, aspirin, and ibuprofen. Other disease-modifying antirheumatic drugs (DMARDs) might be added to the patient treatment course for patients who do not respond to NSAIDs. DMARDs, such as sulfasalazine, may include local steroid injections to reduce stiffness, inflammation, and other discomforts. Prolonged use of medications causes severe reactions, liver cirrhosis, kidney failure, gastrointestinal bleeding, peptic ulcers, hepatorenal damage, and cardiovascular events such as MI.
TNFα antagonists
Tumor necrosis factor-alpha is a physical blocker that is often referred to as an “antagonist.” These TNFα antagonists include biological therapies such as infliximab, etanercept, adalimumab, and golimumab. Biologic medications such as interleukin 17 inhibitors & TNF blockers can trick the immune system to stop or slow down the inflammation process; however, the course of inhibiting the production of proinflammatory cytokines such as IL-17, IL-22, IFN-γ, and TNFα can result in severe side effects and, for some patients, reactivate tuberculosis or make patients more prone to getting new infections.
Surgical Treatment of Bamboo Spine
Due to advances in medicine, surgery is rarely used today. However, surgery might be required for some late-stage cases if pain or extreme swelling occurs rapidly. Surgeries would primarily aim to replace damaged joints with artificial ones. Such surgeries are prevalent in knee replacement and total hip replacement surgeries. Correction surgeries are also needed for patients with severe flexion deformities (downward curvature in the spine), particularly in the cervical spine (neck).
Risks of Surgery
Joint replacement surgeries are inherently risky and temporary, as artificial joints need replacement over time. In addition, the preparation for surgery requiring general anesthesia makes the procedure even more complex to the risk of surgery. Any abrupt changes in the upper airway can lead to difficulties with airway intubation. In some cases, direct spinal or epidural anesthesia may be impossible due to extensive calcification of the damaged ligaments. Stiffness of the thoracic ribs can decrease pulmonary function or result in aortic insufficiency.
TREATMENT RISKS & PRECAUTIONS
Please note that not all patients are good candidates for treating Ankylosing Spondylitis with stem cells. Patients with late-stage, severe underlying conditions, multiple comorbidities, or vision loss (iritis or uveitis) may not qualify for the estimated 2-week treatment protocolStem Cell Treatment for Ankylosing Spondylitis
In the last two decades, considerable progress has been made in the regenerative treatment of spondyloarthritis.
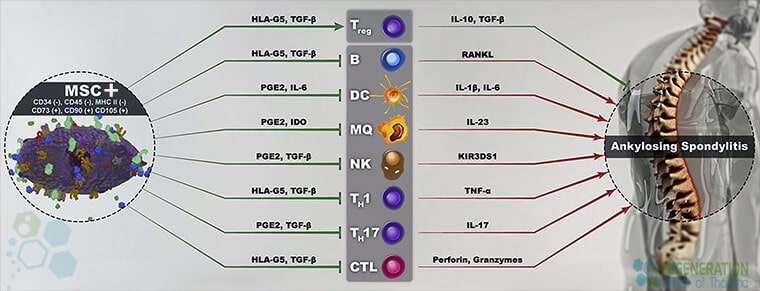
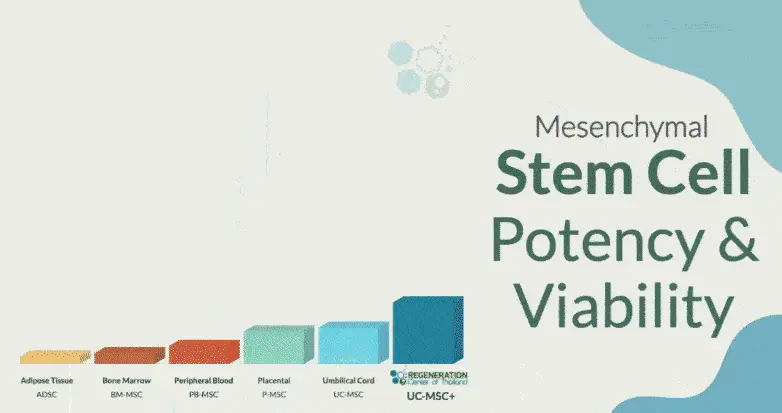
The Regeneration Center Enhanced mesenchymal (UC-MSC+) protocol includes a proprietary combination of adult mesenchymal stem cells, osteoblast-specific growth factors, adipocytes, and chondroblasts with ≥95% cell surface proteins consisting of CD90, CD73, and CD105 markers. Learn more about stem cell therapy. We offer a viable treatment option for patients who are unresponsive to traditional treatments. UC-MSC+ cells offer significant regenerative and immunomodulatory properties that can help reduce inflammatory responses and help repair surrounding tissues via the secretion of soluble factors provided with the growth factors during treatment.[5]
For the treatment of immune-mediated inflammatory disease, the Regeneration Center has developed a unique combination therapy using hematopoietic stem cells and UC-MSC+ cells, which are particularly effective in stabilizing an otherwise abnormal rate of osteogenic differentiation. Learn about how we treat ibm muscle disease with stem cells.
UC-MSC+ cells are engineered to provide low immunogenicity and immunomodulatory properties. UC-MSCs+ therapy for Ankylosing spondylitis does not require immunosuppressive medications. UC-MSC+ cells do not express HLA-DR, making them an ideal therapeutic cell source for transplantation in patients with immune-mediated disorders. UC-MSC+ can eradicate dysfunctional cells and restore immune homeostasis by replacing damaged cells with differentiated B and T cells required for immune homeostasis.[4]
The Regeneration Center Protocol for AS
Total Number of MSC+ Cell Infusions: Total Endogenous Cell Count and range of growth factors will vary based on patient needs.
Types of Stem Cells and Delivery Methods: For patients with moderate AS, multiple sessions of clinical grade expanded UC-MSC+ Mesenchymal Cells along with our proprietary mix of growth factors that can include Bone Morphogenetic Proteins (BMPs), Insulin-like Growth Factor-1 (IGF-1), Transforming Growth Factor-beta (TGF-β), Platelet-Derived Growth Factors (PDGF), Connective Tissue Growth Factors (CTGF), Epidermal Growth Factors (EGF), Vascular Endothelial Growth Factors (VEGF), Fibroblast Growth Factors (FGF) and Nerve Growth Factors (NGF). The regenerative therapy protocol we recommend will depend on the patient’s medical needs. Isolated cells and growth factors are delivered via intravenous drips, direct local injections, intradiscal injections, intrathecal injections, fluoroscopy-guided stem cell delivery (in a hospital setting only), or a combination of these methods to achieve optimal results.
Rehabilitation Post-Treatment: Physical Rehabilitation in Bangkok is optional but strongly recommended. Complete physical rehab services post-therapy can be provided upon request for 2-3 hours per day and up to 5 days per week.
Total Treatment Time Required is estimated to be around two weeks (depending on the type and severity of the condition). Medical and travel visas for extended accommodations at a hotel or apartment for the patient and family can also be provided upon request.
Spondyloarthritis Treatment Guidelines & Requirements
The Regen Center UC-MSC+ Stem Cell treatment for spinal arthritis and Ankylosing spondylitis will require 10-14 days total. Given the varying severity, our medical team must evaluate patients using the current medical records. Evaluations can be done in person or online (submitting documents online). After completion of the medical review, we will provide recommendations, including a detailed treatment plan, specifying the exact number of nights required and the total medical costs for the treatment of ankylosing spondylitis with UC-MSC+ stem cells. Please prepare all current medical records and contact us today to begin the evaluation process.
Published Clinical Citations
[1] ^Chiowchanwisawakit, P., Thaweeratthakul, P., Wattanamongkolsil, L., Srinonprasert, V., Koolvisoot, A., Muangchan, C., Nilganuwong, S., Arromdee, E., & Katchamart, W. (2019). Relationship Between Health-Related Quality of Life and Patient Acceptable Symptom State With Disease Activity and Functional Status in Patients With Ankylosing Spondylitis in Thailand. Journal of clinical rheumatology : practical reports on rheumatic & musculoskeletal diseases, 25(1), 16–23. https://doi.org/10.1097/RHU.0000000000000750
[2] ^ Luft F. C. (2017). Mesenchymal stem cells provide novel insights into ankylosing spondylitis. Journal of molecular medicine, 95(2), 119–121. https://doi.org/10.1007/s00109-016-1496-y
[3] ^Chiowchanwisawakit, P., Pithukpakorn, M., Luangtrakool, K., & Permpikul, P. (2021). HLA-B*27:04 associated with enthesitis and younger age of onset, and HLA-B allele profile in patients with ankylosing spondylitis in Thailand: A cross-sectional study. International journal of rheumatic diseases, 24(3), 411–417. https://pubmed.ncbi.nlm.nih.gov/33448675/
[4] ^Abdolmohammadi, K., Pakdel, F. D., Aghaei, H., Assadiasl, S., Fatahi, Y., Rouzbahani, N. H., Rezaiemanesh, A., Soleimani, M., Tayebi, L., & Nicknam, M. H. (2019). Ankylosing spondylitis and mesenchymal stromal/stem cell therapy: a new therapeutic approach. Biomedicine & pharmacotherapy = Biomedecine & pharmacotherapie, 109, 1196–1205. https://doi.org/10.1016/j.biopha.2018.10.137
[5] ^ Zheng, G., Xie, Z., Wang, P., Li, J., Li, M., Cen, S., Tang, S., Liu, W., Ye, G., Li, Y., Wang, S., Wu, X., Su, H., Wu, Y., & Shen, H. (2019). Enhanced osteogenic differentiation of mesenchymal stem cells in ankylosing spondylitis: a study based on a three-dimensional biomimetic environment. Cell death & disease, 10(5), 350. https://doi.org/10.1038/s41419-019-1586-1