

Knee arthritis is a progressive degenerative condition affecting millions worldwide, characterized by cartilage degeneration, synovial inflammation, and eventual joint dysfunction. Current diagnostic protocols identify multiple arthritis variants through clinical examination and imaging studies. Traditional therapeutic interventions often provide temporary symptomatic relief but fail to address underlying tissue damage, underscoring the need for stem cell infusion strategies using culture-expanded mesenchymal stem cells for osteoarthritis. Recent advances in regenerative medicine, particularly mesenchymal stem cell therapy, demonstrate significant potential for cartilage restoration and modulation of inflammation in patients with knee osteoarthritis. These emerging treatment modalities may fundamentally alter the therapeutic landscape for arthritic joint conditions, especially through the integration of mesenchymal stem cells for knee injuries.
Understanding Knee Arthritis: Types and Overview
While knee arthritis is one of the most prevalent musculoskeletal disorders affecting millions worldwide, it encompasses several distinct pathophysiological processes that warrant precise clinical differentiation. Osteoarthritis, the most prevalent form, is characterized by the progressive degeneration of joint structures due to mechanical wear and compromised cartilage integrity, necessitating treatment. This degenerative process typically affects weight-bearing surfaces and meniscal tissues.
Related joint pathology: Similar degenerative and inflammatory mechanisms affect the shoulder complex, especially the glenohumeral joint and rotator cuff tendons, and hip joints. If you’re researching tendon-driven shoulder pain or partial-thickness tears.
- Rheumatoid arthritis, Connective tissue disease, and myasthenia gravis are autoimmune conditions characterized by systemic inflammatory processes that target synovial membranes, often leading to pain and functional impairment. The resulting synovitis produces destructive enzymes that erode cartilage and subchondral bone, further complicating treatment of osteoarthritis.
- Post-traumatic arthritis develops following acute brain injuries, spinal injuries, burst fractures, or repetitive microtrauma, accelerating normal deteriorative changes, which may be mitigated by physical therapy and early intervention.[1]
- Psoriatic arthritis, Ankylosing Spondylitis, hand injuries, and other spondyloarthropathies demonstrate asymmetric joint involvement with distinct radiographic patterns, complicating treatment for osteoarthritis.
- Enteropathic Arthritis is another type of arthritis associated with inflammatory bowel diseases, such as ulcerative colitis and Crohn’s disease.
- Septic arthritis requires immediate intervention to prevent irreversible joint destruction, and timely application of stem cell injections for osteoarthritis may be a future consideration in treatment protocols.
Each arthritis subtype demonstrates unique clinical presentations, diagnostic markers, and treatment protocols. Accurate classification enables The Regeneration Center to implement targeted therapeutic strategies that optimize patient outcomes and preserve functional mobility for those seeking exhaustive care.
Early Warning Signs of Knee Arthritis
Although knee arthritis progression occurs gradually over months to years, specific prodromal symptoms consistently emerge, enabling early clinical detection and intervention. Healthcare professionals must recognize these initial manifestations to implement appropriate pain management strategies and preserve patient function, particularly in cases that require a systematic review of treatment options.
Morning joint stiffness represents the primary early indicator, typically lasting 15-30 minutes upon awakening. Patients often experience difficulty initiating movement, particularly when rising from a seated position or from bed, which can be improved with targeted interventions such as targeted stem cell infusions. This stiffness gradually diminishes with gentle activity but may recur after prolonged inactivity, particularly in patients with mild-to-moderate knee osteoarthritis.
Reduced mobility becomes apparent through subtle limitations in knee flexion and extension, particularly in patients with knee osteoarthritis. Patients report increased effort required for routine sports activities such as stair climbing, squatting, or prolonged walking. Weight-bearing activities may produce mild discomfort or fatigue. Additional warning signs include intermittent joint swelling, crepitus with movement, and fluctuations in symptoms with weather changes.
As part of the differential, consider spinal stenosis when leg pain or heaviness begins after standing or walking and eases with sitting or bending forward (the “shopping-cart sign”), especially if symptoms are bilateral and include numbness or tingling in the calves or thighs. This pattern is often due to lumbar canal narrowing affecting L4–S1 roots, which differs from joint-line pain and swelling seen in primary knee arthritis and should guide imaging and management. Early identification of these symptoms allows clinicians to initiate conservative treatment protocols, potentially slowing degenerative progression and maintaining ideal joint function for extended periods.[2]
Common Symptoms That Indicate Joint Degeneration
Additional degenerative indicators include crepitus during range-of-motion testing, progressive functional limitations, and compensatory gait patterns, all of which can be assessed in the context of knee osteoarthritis. These symptoms collectively demonstrate the progression of cartilage breakdown, subchondral bone changes, and synovial membrane dysfunction characteristic of knee arthritis. Patients may also experience stiffness, particularly in the morning or after periods of inactivity. This stiffness can reduce the range of motion, making it difficult to perform daily activities.
Other common symptoms include knee joint swelling, which may result from inflammation or fluid accumulation. As the condition progresses, individuals may notice increased pain during weight-bearing activities, such as walking or climbing stairs. The pain may become chronic, persisting even at rest. Patients often report a sensation of instability or a feeling that the knee “gives way,” which can further impair mobility and quality of life.
In addition to physical symptoms, knee arthritis can also have emotional and psychological effects. Chronic pain and reduced mobility can lead to frustration, anxiety, and depression, making it crucial for individuals to seek comprehensive treatment options, including innovative approaches such as stem cell therapy for knee arthritis. This therapy aims to regenerate damaged tissues and reduce inflammation, potentially offering relief from these debilitating symptoms.
Rule-out note: Pain that shoots from the lower back or buttock and travels past the knee (especially with numbness, tingling, or leg weakness) may indicate peripheral neuropathy, L4–S1 radiculopathy from the sciatic nerve or femoral nerve rather than primary knee arthritis.
Primary Causes and Risk Factors of Knee OA
Understanding the etiology of knee arthritis requires examination of both intrinsic and extrinsic factors that contribute to cartilage degeneration and joint dysfunction in patients with knee osteoarthritis. Primary causative mechanisms include genetic predisposition, which influences collagen synthesis, cartilage matrix composition, and patterns of inflammatory response. Age-related degeneration is the most significant intrinsic risk factor, as chondrocyte regenerative capacity declines progressively, resulting in reduced proteoglycan production and compromised cartilage integrity.
Obesity and excess weight are critical extrinsic factors that increase mechanical loading on articular surfaces while promoting systemic inflammation through adipokine release. Additional risk factors encompass previous joint trauma, repetitive occupational stress, anatomical malalignment, and hormonal fluctuations. Secondary arthritis may develop following ligamentous injuries, meniscal tears, or fractures involving articular surfaces. Gender influences prevalence patterns, with postmenopausal women demonstrating increased susceptibility. Metabolic conditions, including diabetes type 2, pancreatitis, ARLD, PSC and gout, further accelerate degenerative processes through inflammatory pathways and crystal deposition within synovial tissues.[3]
Traditional Treatment Approaches, Risks & Limitations
Management strategies for knee arthritis have traditionally focused on symptom mitigation rather than disease modification, employing conservative interventions as first-line therapy before progressing to surgical options. Initial protocols typically include nonsteroidal anti-inflammatory drugs (NSAIDs), corticosteroid injections, and structured rehabilitation programs, plus physical therapy plus hyaluronic acid injection.
However, significant medication limitations emerge with prolonged NSAID use, including gastrointestinal complications, cardiovascular risks, and renal dysfunction. Corticosteroid efficacy diminishes over time, potentially accelerating cartilage degradation, highlighting the need for isolated, expanded stem cell injections for knee osteoarthritis.

Physical therapy constraints include patient compliance challenges, limited efficacy in advanced disease stages, and inability to reverse structural joint damage, which can be addressed with a combination of physical therapy plus hyaluronic acid. While beneficial for maintaining mobility and strength, therapeutic exercises cannot regenerate deteriorated cartilage.
Surgical drawbacks include substantial recovery periods, infection risks, implant failure rates, and limited longevity, all of which may necessitate revision procedures. Total knee arthroplasty, while effective for end-stage disease, is an irreversible intervention with potential complications, including loosening, wear, and reduced range of motion, underscoring the need for innovative treatment modalities.
Stem Cell Therapy for Arthritis is Non-Surgical
Three distinct categories of stem cells demonstrate therapeutic potential for the treatment of knee arthritis: mesenchymal stem cells (MSCs), adipose-derived stem cells (ADSCs) for autologous adipose tissue-derived mesenchymal stem cell therapy, and bone marrow aspirate concentrate (BMAC). These cellular therapies act through paracrine signaling to alleviate joint inflammation by modulating cytokine production and immune responses in the synovial environment.

MSCs exhibit chondrogenic differentiation capacity, enabling direct contribution to improve cartilage regeneration through extracellular matrix synthesis and chondrocyte proliferation. ADSCs, harvested via minimally invasive liposuction procedures, exhibit regenerative properties similar to those of bone marrow-derived alternatives while offering superior accessibility and yield.
Repairing vs Regenerating Cartilage
UC-MSC+ procedures call for concentrated low-passage stem cells and tissue-specific growth factors that are delivered directly to multiple targeted points, promoting endogenous repair mechanisms. These interventions reduce the need for invasive procedures compared to traditional surgical approaches, offering patients viable alternatives to joint replacement surgery. Clinical evidence indicates significant improvements in pain reduction, functional mobility, and cartilage preservation across multiple stem cell modalities for the management of knee osteoarthritis.
How Stem Cell Treatment Works for Knee Arthritis
When stem cells are introduced into arthritic knee joints, they initiate a multi-phase therapeutic cascade that begins with homing to damaged tissues via chemotactic signaling pathways. These pluripotent cells, including bone marrow mesenchymal stem cells and adipose-derived mesenchymal stem cells, differentiate into chondrocytes, osteoblasts, and other specialized cell types essential for structural restoration. Cell-based healing occurs through paracrine signaling, which releases anti-inflammatory cytokines, growth factors, and immunomodulatory proteins, potentially enhanced by stem cells for the treatment of knee osteoarthritis.[4]
The therapeutic process involves three primary mechanisms, including the application of stem cells, such as mesenchymal stem cell injections, for the treatment of knee osteoarthritis. First, direct cellular replacement occurs as stem cells transform into functional cartilage and bone cells. Second, cartilage regeneration advances through enhanced collagen synthesis and proteoglycan production within the extracellular matrix. Third, extensive tissue repair involves angiogenesis, reduced levels of inflammatory markers, and improved synovial fluid composition.
TREATMENT RISKS & PRECAUTIONS
Please note that not all patients are suitable candidates for stem cell therapy for Osteoarthritis of the Knees. Patients with advanced joint damage, severe deformities, previous surgeries, or other significant health issues may not be good candidates for treatment.Natural Cartilage Regeneration
Clinical outcomes demonstrate significant improvements in joint function, pain reduction, and structural integrity. Mesenchymal stem cells show particular efficacy in treating knee arthritis, with patients experiencing improved mobility and reduced degenerative progression through sustained regenerative activity. This innovative approach leverages the body’s natural healing mechanisms to regenerate damaged cartilage and improve overall joint health. Numerous studies have shown that stem cell therapy can effectively reduce inflammation and promote tissue repair, leading to long-lasting relief from arthritis symptoms. Furthermore, the minimally invasive nature of these procedures makes them an attractive option for patients looking to avoid traditional surgical interventions. As research continues to evolve, the potential of stem cell therapy for knee arthritis appears promising, with ongoing trials aimed at optimizing treatment protocols and understanding the long-term benefits of this regenerative treatment of osteoarthritis.
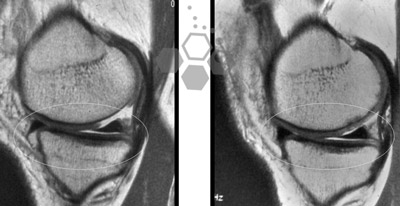
Before After Stem Cells for Knee Arthritis

The Regeneration Center Difference
While the mechanisms of stem cell therapy remain consistent across treatment facilities, The Regeneration Center distinguishes itself through the development of proprietary protocols that optimize cellular viability and therapeutic outcomes. The facility implements advanced cryopreservation techniques and specialized processing methods to maintain mesenchymal stem cell potency throughout cultivation and administration, ensuring optimal outcomes in stem cell injection therapies.[5]
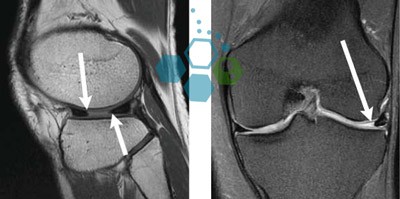
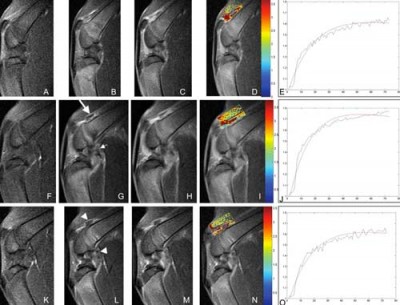
The Center’s patient-centered approach encompasses thorough assessments utilizing advanced imaging modalities, synovial fluid analysis, and biomechanical evaluation protocols. These diagnostic procedures enable clinicians to quantify the severity of cartilage degradation, identify inflammatory biomarkers, and assess joint stability parameters.
Individualized treatment plans incorporate patient-specific variables, including age, comorbidities, activity levels, and arthritis classification staging. Treatment protocols adjust stem cell dosages, injection techniques, and adjunctive therapies, including mesenchymal stem cell injection plus physical therapy, accordingly. Our facility employs ultrasound-guided intra-articular delivery systems to ensure precise cellular placement within affected joint compartments. Post-treatment monitoring includes serial MRI assessments, functional outcome measures, and biomarker tracking to assess regenerative progress and optimize rehabilitation protocols to enhance therapeutic efficacy.
Clear evidence demonstrates that stem cell therapy’s efficacy in treating knee arthritis through cartilage regeneration, modulation of inflammation, and enhanced proteoglycan synthesis, particularly with targeted UC-MSC stem cell infusions. Our clinical outcomes indicate significant improvements in joint function, reduced pain, and slower degenerative progression compared with conventional interventions, particularly when targeted stem cell injection techniques are incorporated. The therapeutic mechanism involves stem cell differentiation into chondrocytes, thereby promoting tissue repair and restoring synovial homeostasis using intra-articular injection of mesenchymal stem cells essential for the treatment of knee osteoarthritis. Advanced regenerative protocols represent a paradigm shift from symptomatic management to targeted tissue restoration in arthritic joint pathology.
Cost of Stem Cell Treatment for Knee Osteoarthritis in 2026
UC-MSC+ Stem Cell treatment for Knee Arthritis and degenerative knee joint disease will require an estimated 10-14 days. Given the varying degrees of severity, our orthopedic team will need to review the patient’s medical records and radiologic scans to establish an appropriate protocol. Upon completion of the medical review, detailed treatment recommendations will be provided, including the specific cell types, delivery methods, the exact number of required days, and the total medical-related costs. To begin the evaluation process for our multi-stage knee arthritis treatment protocol using targeted intra-articular infusion, please prepare your recent medical records, such as MRI scans of the knees, and contact us today.
Published Clinical Citations
[1] ^ Wei P, Bao R. Intra-Articular Mesenchymal Stem Cell Injection for Knee Osteoarthritis: Mechanisms and Clinical Evidence. Int J Mol Sci. 2022 Dec 21;24(1):59. doi: 10.3390/ijms24010059. PMID: 36613502; PMCID: PMC9819973.
[2] ^ Sriwatananukulkit O, Tawonsawatruk T, Rattanapinyopituk K, Luangwattanawilai T, Srikaew N, Hemstapat R. Scaffold-Free Cartilage Construct from Infrapatellar Fat Pad Stem Cells for Cartilage Restoration in Thailand. Tissue Eng Part A. 2022 Mar;28(5-6):199-211. doi: 10.1089/ten.TEA.2020.0167. Epub 2020 Oct 23. PMID: 32972295.
[3] ^ Kasemkijwattana C, Hongeng S, Kesprayura S, Rungsinaporn V, Chaipinyo K, Chansiri K. Autologous bone marrow mesenchymal stem cells implantation for cartilage defects: two cases report. J Med Assoc Thailand. 2011 Mar;94(3):395-400. PMID: 2156084
[4] ^Filippo M, Laura M, Riccardo G, Valeria V, Eschweiler J, Maffulli N. Mesenchymal stem cells augmentation for surgical procedures in patients with symptomatic chondral defects of the knee: a systematic review. J Orthop Surg Res. 2022 Sep 14;17(1):415. doi: 10.1186/s13018-022-03311-1. PMID: 36104803; PMCID: PMC9476260.
[5] ^ Gadelkarim M, Abd Elmegeed A, Allam AH, Awad AK, Shehata MA, AbouEl-Enein A, Alsadek ME, Abo Deeb M, Afifi AM. Safety and efficacy of adipose-derived mesenchymal stem cells for knee osteoarthritis: A systematic review and m-analysis. Joint Bone Spine. 2022 Oct;89(5):105404. doi: 10.1016/j.jbspin.2022.105404. Epub 2022 May 6. PMID: 35534001.