
A Brain stem injury can occur via blunt force trauma to the brain, no matter the age at onset. A head injury can result in a substantial handicap to the individual who sustained the brain injury and may trigger numerous types of cognitive impairments, such as lack of focus, memory, or other motor-neurological disorders, such as ataxia, ALS, Spinal muscular atrophy, PSP or Parkinson’s Disease. This is why stem cell treatment for CSVD-related vascular brain injury belongs in a separate review from traumatic brain injury, concussion, and blunt-force head trauma.
Etiology of Traumatic Brain Injury
Modern treatment options for head injuries are usually divided into two types: closed-head injuries and penetrating head injuries. Overlap for the two types does exist, and closed head injury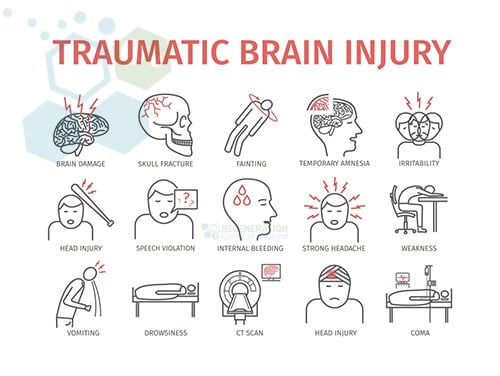 treatments can be further segmented into mild, moderate, or severe/traumatic head injuries. A neurological injury is dissimilar from a traumatic brain injury (TBI) or stroke because an exterior force injures the brain in a damaging, violent manner. TBI is an injury to the brain caused by a traumatic event. TBI and brain damage can be caused by blows to the head (severe head trauma), cerebral trauma, cranial penetration, or even violent trembling. Depending on the cause and severity of the trauma, brain damage can be classified as severe, moderate, or mild, and damage from neurodegeneration can include glial cells, neurons, endothelial cells, and Axonal Degeneration. [1]
treatments can be further segmented into mild, moderate, or severe/traumatic head injuries. A neurological injury is dissimilar from a traumatic brain injury (TBI) or stroke because an exterior force injures the brain in a damaging, violent manner. TBI is an injury to the brain caused by a traumatic event. TBI and brain damage can be caused by blows to the head (severe head trauma), cerebral trauma, cranial penetration, or even violent trembling. Depending on the cause and severity of the trauma, brain damage can be classified as severe, moderate, or mild, and damage from neurodegeneration can include glial cells, neurons, endothelial cells, and Axonal Degeneration. [1]
Classifications of Traumatic Brain Injuries (TBI)
A TBI occurs after damage to the brain from external forces such as Impacts, rapid deceleration or acceleration, blast 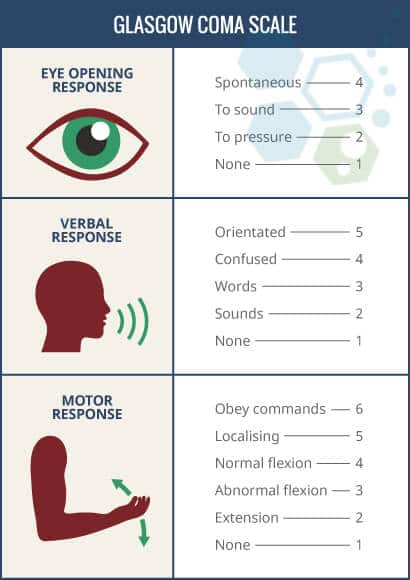 waves, or blunt force trauma. After such an incident, overall neurological impairment can be temporary or permanent, depending on the severity of blunt force trauma to the head. The focus of this article will be to understand the signs, symptoms, and new treatment options for traumatic head injuries that occur after birth, especially those following traumatic brain injury. There are currently two subsets of brain damage, including traumatic and non-traumatic (non-penetrating) brain injuries resulting from exposure to toxins, brain stroke, or viral infections. Most brain injuries are classified as either neurotrauma or central nervous system injuries that can affect cell signaling and neurotransmitters, which can lead to other neurodegenerative conditions like dementia. Recent medical studies also indicate that inflammatory responses following traumatic brain injury and autoimmune processes are significant factors that lead patients from TBI events to eventual permanent loss of cognitive capabilities.
waves, or blunt force trauma. After such an incident, overall neurological impairment can be temporary or permanent, depending on the severity of blunt force trauma to the head. The focus of this article will be to understand the signs, symptoms, and new treatment options for traumatic head injuries that occur after birth, especially those following traumatic brain injury. There are currently two subsets of brain damage, including traumatic and non-traumatic (non-penetrating) brain injuries resulting from exposure to toxins, brain stroke, or viral infections. Most brain injuries are classified as either neurotrauma or central nervous system injuries that can affect cell signaling and neurotransmitters, which can lead to other neurodegenerative conditions like dementia. Recent medical studies also indicate that inflammatory responses following traumatic brain injury and autoimmune processes are significant factors that lead patients from TBI events to eventual permanent loss of cognitive capabilities.
TBI is classified based on several factors, including severity, causative forces, anatomical locations of the Injury, and the mechanism. Mechanism-related injuries are either considered penetrating head injuries or nonpenetrating/blunt/closed Injuries. An open or penetrating head injury happens when an object goes through the skull and breaches the outermost membrane of the brain, known as the dura mater.
Glasgow Coma Scale – GCS
Traumatic Brain injuries are classified into three categories: mild, moderate, and severe. The most commonly used system around the world to classify TBI severity is known as The Glasgow Coma Scale (GCS). The GCS scale (3–15) grades a patient based on their level of consciousness, which is assessed through motor, verbal, and eye-opening responses. A brain injury with a GCS of 13 or above is considered mild, a head injury with a GCS score of 9–12 is deemed moderate, and any GCS score below eight is considered a severe head injury.
The GCS scale can also be changed after the victim is resuscitated, after post-traumatic amnesia (PTA), or after recovering from the loss of consciousness (LOC). Other methods of classifying the severity of TBI include using neuroimaging scans (CT, MRI, or PET) to measure brain swelling, diffuse Injury, or focal lesions. A mild TBI is also commonly known as a concussion, but such an injury results in brain contusion or leads to trauma-induced paralysis.
Stem Cells Used in Cases with Anoxic Brain Damage
Each region of the human brain and spinal cord contains specialized cells, including several cell types involved in the treatment of traumatic brain injury. The Regen Center NeuroCell protocol uses adult MSC+ cells isolated and differentiated into neural, glial, and Astrocytes. These are crucial cell types involved in the brain’s response following traumatic brain injury and are needed for specific regions that help develop the central nervous system (CNS).
Our neural cell replacement therapy for spinal cord injuries targets damaged areas and then repairs dead or diseased progenitor cells in the neurogenic region.
Initial symptoms and signs of the TBI could consist of:
- Headaches
- Blurred vision
- Dizziness
- Confusion
- Seizures
- Memory loss
- CRPS
- Loss of consciousness
- Paralysis or severe traumatic brain injury can lead to significant long-term disabilities and severe movement disorders
- Coma
Focal vs. Diffuse Brain Injuries
Using a CT scan, TBI lesions can also be classified by their pathological features, including extra-axial or intra-axial. Extra-axial lesions refer to injuries outside the brain but inside the skull, while intra-axial lesions refer to injuries inside the brain tissue. Depending on the severity, results from these injuries can be diffuse, focal, or both.
Warning Symptoms After Traumatic Brain Injury
Symptoms of Diffuse injuries include edema (brain swelling) and destruction to white matter tracts, cerebral hemispheres, and axons (diffuse axonal). Focal injuries, on the other hand, occur primarily in the orbitofrontal cortex and temporal lobes, resulting in behavioral changes, decision-making difficulties, and language problems.
Focal lesions, such as Hematomas, result in rapid accumulation of blood around the brain. They can result in Intracerebral hemorrhage stroke, subdural hematoma (bleeding between the arachnoid membrane and the dura mater), subarachnoid hemorrhage (bleeding between the arachnoid membrane and the pia mater), aphasia, epidural hematoma (bleeding into the dura mater), or intraventricular hemorrhage (bleeding in the ventricles).
Stem Cell Treatment for TBI after Blunt Force Trauma
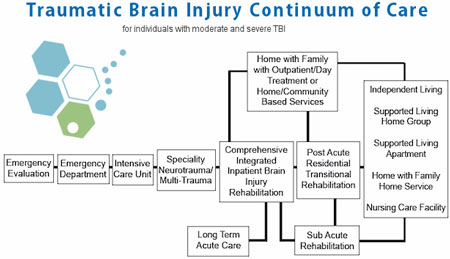
Early intervention is key to optimal recovery from brain injuries that affect the nervous system. Response during the first 60 minutes after Injury, i.e., “golden hour,” is recommended.[2] For most patients, treatment options depend on the age of the Injury and stage of recovery. Patients in the acute phase are looking to stabilize the condition from progressing using a combination of surgery, physical rehabilitation, and therapy for traumatic brain injury.
For Acute stages of TBI or injuries that occurred while playing sports, maintaining proper blood flow to the brain is critical to avoid brain herniation and seizures. In this stage, a Decompressive craniectomy (DC) can be used to relieve intracranial pressure, along with hyperbaric oxygen therapy to ensure adequate oxygen supply. Neuroimaging from brain scans is also used to guide the use of analgesics, Sedatives, paralytic agents, and, in some cases, hypertonic saline to reduce swelling, regulate body temperature and blood pressure, reduce the risk of heart failure, treat brain fog, and prevent electrolyte imbalances.
Patients with TBI are at a much higher risk of complications and adverse side effects, requiring continuous monitoring for signs of deterioration or loss of consciousness. Other complications of traumatic brain injury include pulmonary edema and cardiac arrhythmia. In chronic stages of TBI, pharmacological-based treatments can be used to treat behavioral (psychiatric issues) and post-traumatic epilepsy. Learn about the best food for your brain.
Reverse Damage From Brain Injury – Stop Concussions
Brain Stem cell transplantation into the affected region might be beneficial in certain circumstances, such as when the damage is not too severe and occurred relatively recently. (from 6 months up to two years after initial Injury) The purpose of neural stem cell implantation is to restore signal function with properties similar to those of the original signals. In TBI, numerous cell types (glial, neuronal, vascular, and endothelial) are required to regenerate the complex functions of largely damaged brain regions.[3]
Neural Cell Replacement Therapy
In much more severe instances of traumatic brain-related injuries, such as Chronic traumatic encephalopathy (CTE), some complications can be fatal. While the rigorousness of the TBI
Though the severity of traumatic brain injury differs broadly, the consequences of it, in the long run, are frequently devastating and life-changing for the injured brain. TBI is typically sudden, and early intervention is key to full recovery. The physical, non-congenital harm to the brain by an external force may permanently or temporarily disrupt regular brain function, often seen in patients following traumatic brain injury. [4] Brain characteristics and functions that may be affected include temporary or permanent loss of consciousness, speech, language, memory, character, mobility, joint pain with lupus, peripheral neuropathy, and recognition of other people. Since the brain controls all bodily functions, any harm to the brain (neurons) can impair physical and psychological function, whether minor or severe.[5]
TREATMENT RISKS & PRECAUTIONS
Please note that not all patients are suitable candidates for treating brain injuries with stem cells. Patients with extensive brain damage, severe cognitive impairment, or other critical health issues might not be good candidates for treatment.Stem Cell Treatment For TBI
Total Number of MSC+ Cell Sessions Needed: For most patients, we will need multiple Infusions of isolated and expanded mesenchymal cells, which can be cultured from autologous bone marrow (BMMSC) or allogeneic sources (UC-MSC) and Neural Stem cells (MSC–NSC). These stem cells and our proprietary combination of growth factors are combined to enhance the treatment’s therapeutic potential. The growth factors we isolate and culture are naturally occurring proteins in cells that stimulate cell growth, proliferation, healing, and differentiation, and are combined with stem cells to support brain repair and regeneration. Some of the growth factors we isolate for TBI patients include Brain-Derived Neurotrophic Factor (BDNF), Nerve Growth Factor (NGF), Epidermal Growth Factor (EGF), Vascular Endothelial Growth Factor (VEGF), Fibroblast Growth Factors (FGFs), Insulin-like Growth Factor 1 (IGF-1), and Glial Cell Line-Derived Neurotrophic Factor (GDNF)
Delivery Methods for MSC+ and Neural Stem Cells: The types of cellular infusions will vary based on patient needs. However, our treatment aims to reduce systemic neuroinflammation and promote faster recovery of lost cognitive function through neurogenesis in most cases of acute brainstem injury. To achieve these results, cells can be administered via a combination of Intravenous infusions, stereotactic-guided delivery, inhalation therapy with micro-nebulized mesenchymal cells, Intrathecal infusions, and fluoroscopy-guided cell delivery (in a hospital setting only). All intrathecal injections at The Regeneration Center are done by a board-certified neurosurgeon and are needed to bypass the blood-brain barrier. Restoring the blood-brain barrier (BBB) can be a crucial component of treatment, as it plays a vital role in maintaining brain homeostasis and protecting it from harmful substances.
Clinical Rehabilitation Post-Treatment: Physical Rehabilitation therapy in Bangkok is optional, depending on the patients’ travel/time constraints. Complete physical rehabilitation post-therapy can be provided upon request, for 2-4 hours per day, up to 5 days per week. Medical visas and extended-stay accommodations for the patient and family may also be included upon request.
Cost of Treating Brain Injuries with Stem Cells & Physical Rehab
The Regeneration Center stem cell treatment for Traumatic Brain Injuries will require a minimum of 2 weeks in Bangkok, focusing on mesenchymal stem cell transplantation for the injured brain. Due to significant differences in treatment requests for brain injury, our medical team must assess the potential candidate’s eligibility for treatment. Upon acceptance, a detailed treatment plan will be provided, specifying the total number of nights required and the total medical-related expenses (excluding accommodations or flights), including cell extraction, enrichment, and infusions. To begin the qualification process for multi-stage TBI neural stem cell transplants, please prepare your recent medical records, such as recent Brain MRIs, CT scans (Preferred), or PET Scans, and contact us today.
Published Clinical Citations
[1] ^ Dharmasaroja, Permphan. 2008. Bone marrow-derived mesenchymal stem cells for the treatment of ischemic stroke. Journal of Clinical Neuroscience : Official Journal of the Neurosurgical Society of Australasia, no. 1 (November 18). doi:10.1016/j.jocn.2008.05.006. https://www.ncbi.nlm.nih.gov/pubmed/19017556
[2] ^ Dinh, Michael M, Kendall Bein, Susan Roncal, Christopher M Byrne, Jeffrey Petchell, and Jeffrey Brennan. 2012. Redefining the golden hour for severe head injury in an urban setting: the effect of prehospital arrival times on patient outcomes. Injury, no. 5 (February 14). doi:10.1016/j.injury.2012.01.011. https://www.ncbi.nlm.nih.gov/pubmed/22336130
[3] ^ Kunkanjanawan, Tanut, Parinya Noisa, and Rangsun Parnpai. Modeling neurological disorders by human induced pluripotent stem cells in Thailand Journal of biomedicine & biotechnology (November 24). doi:10.1155/2011/350131. https://www.ncbi.nlm.nih.gov/pubmed/22162635
[4] ^ Prè, Deborah, Michael W Nestor, Andrew A Sproul, Samson Jacob, Peter Koppensteiner, Vorapin Chinchalongporn, Matthew Zimmer, Ai Yamamoto, Scott A Noggle, and Ottavio Arancio. 2014. A time course analysis of the electrophysiological properties of neurons differentiated from human induced pluripotent stem cells (iPSCs). PloS one, no. 7 (July 29). doi:10.1371/journal.pone.0103418. https://www.ncbi.nlm.nih.gov/pubmed/25072157
[5] ^ Yang, Yongxiang, Yuqin Ye, Xinhong Su, Jun He, Wei Bai, and Xiaosheng He. 2017. MSCs-Derived Exosomes and Neuroinflammation, Neurogenesis and Therapy of Traumatic Brain Injury. Frontiers in cellular neuroscience (February 28). doi:10.3389/fncel.2017.00055. https://www.ncbi.nlm.nih.gov/pubmed/28293177