
Progressive supranuclear palsy (PSP) is one of the most difficult tauopathies to identify early because its first symptoms can resemble Parkinson’s disease, age-related imbalance, or even a primary visual problem. For a website that already covers a wide spectrum of neurological and spinal conditions, PSP warrants its own focused explanation because it simultaneously affects gait, eye movements, swallowing, speech, behavior, and executive function.
It also belongs within the larger conversation about atypical Parkinsonism and other movement disorders. That broader context matters because many patients spend months or years being treated for a more familiar diagnosis before the hallmark pattern of vertical gaze limitation, early backward falls, and axial rigidity becomes obvious.
What Is Progressive Supranuclear Palsy?
Progressive supranuclear palsy is a rare, progressive, four-repeat tauopathy in which abnormal tau accumulates in neurons and glia, particularly in the brainstem, basal ganglia, and frontal cortical networks. As these regions degenerate, patients lose the smooth integration required for posture, balance, visual tracking, speech initiation, swallowing, and higher-order cognitive control[1].
Although PSP is classified as an atypical Parkinsonian disorder, it is not simply a faster form of Parkinson’s disease. Tremor is often minimal or absent; stiffness tends to affect the neck and trunk more than the hands; and the characteristic eye-movement disorder can become as disabling as gait impairment. The clinical picture is also broader than pure motor dysfunction because frontal lobe involvement may cause apathy, slowed thinking, reduced verbal fluency, or impulsive behavior.
Clinicians may encounter several phenotypes, including the classic Richardson syndrome presentation and more Parkinson-like variants that initially respond to levodopa. That variability is one reason PSP is frequently underrecognized in its earliest stage.
Early Signs and Symptoms of PSP
Early PSP symptoms often start with subtle changes that patients describe as clumsiness, unexplained imbalance, or a growing fear of stairs and curbs. The classic fall pattern is 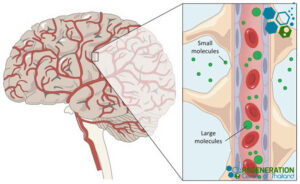 backward rather than forward, reflecting axial postural instability and impaired postural reflexes. In many cases, family members notice that the patient looks stiff in the neck and shoulders, turns the whole body instead of pivoting smoothly, or hesitates when changing direction.
backward rather than forward, reflecting axial postural instability and impaired postural reflexes. In many cases, family members notice that the patient looks stiff in the neck and shoulders, turns the whole body instead of pivoting smoothly, or hesitates when changing direction.
Visual symptoms are equally important. Slowed vertical saccades, difficulty looking down, double vision, and eventual vertical supranuclear gaze palsy may appear before a classic diagnosis is made. Because looking downward becomes difficult, patients may misjudge plate edges, steps, and floor obstacles, which directly adds to fall risk.
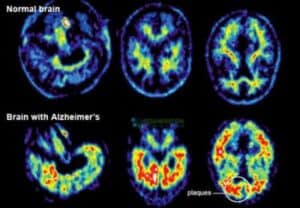
Bulbar and cognitive symptoms often follow. Speech may become strained, slurred, or low in volume, while swallowing may become slow enough to increase the risk of choking and aspiration. Executive dysfunction, emotional lability, apathy, and reduced mental flexibility can make the condition look less like a pure movement disorder and more like Alzheimer’s, vascular, and Lewy body dementia in its later stages, especially when caregivers focus on the cognitive decline more than the eye movement findings.
Why PSP Is Often Misdiagnosed as Parkinson’s
PSP is often misdiagnosed as Parkinson’s in the beginning because both conditions can present with bradykinesia, muscular rigidity, reduced facial expression, and gait slowing. The confusion is even greater in PSP-parkinsonism, where a patient may show a modest early response to dopaminergic medication and may not yet have a dramatic gaze palsy [2].
The differentiating pattern becomes clearer when clinicians look for several features together rather than relying on a single symptom. PSP is more suspicious when the onset is relatively symmetric, the stiffness is mainly axial, the patient falls early, tremor is not prominent, eye movements are slow vertically, and any medication response is incomplete or short-lived. Earlier dysarthria, dysphagia, eyelid opening difficulty, and frontal behavioral change also support the diagnosis.
That distinction matters clinically. A patient labeled with idiopathic Parkinson’s disease may spend valuable time escalating symptomatic therapy, while the real priority in PSP should be fall prevention, swallowing surveillance, realistic counseling, and early multidisciplinary support.
How PSP Is Diagnosed
There is no single blood test that confirms PSP, so diagnosis remains primarily clinical. A movement-disorder neurologist usually combines bedside examination of vertical saccades, postural stability, gait initiation, axial tone, speech, and cognition with a careful history of when falls, visual symptoms, and swallowing problems first began.
Brain MRI is usually performed to support the workup and to exclude mimics, rather than as a standalone diagnostic test. In patients with cognitive decline, gait changes, and vascular imaging findings, clinicians may also consider CSVD and vascular dementia overlap before assuming every symptom is caused by PSP alone. In some patients, it may show midbrain atrophy or other supportive patterns, but it is just as important for ruling out structural explanations such as ischemic or hemorrhagic stroke that can produce overlapping problems with gait, gaze, or executive function.
A prior traumatic brain injury can further complicate the picture because head trauma may leave lasting deficits in balance, visual tracking, attention, or speech. For that reason, the most useful workup usually includes swallowing assessment, speech evaluation, fall history, medication review, and sometimes formal neuropsychological testing rather than relying on imaging alone.
PSP Causes and Risk Factors
 The exact cause of PSP remains incompletely understood, but its core pathology is abnormal tau aggregation. In affected brain regions, hyperphosphorylated four-repeat tau disrupts intracellular transport, destabilizes neuronal function, activates glial responses, and contributes to progressive cell loss. Over time, this produces a network disorder rather than a single-region lesion, which explains why motor, ocular, cognitive, and bulbar symptoms can all evolve together.
The exact cause of PSP remains incompletely understood, but its core pathology is abnormal tau aggregation. In affected brain regions, hyperphosphorylated four-repeat tau disrupts intracellular transport, destabilizes neuronal function, activates glial responses, and contributes to progressive cell loss. Over time, this produces a network disorder rather than a single-region lesion, which explains why motor, ocular, cognitive, and bulbar symptoms can all evolve together.
Most cases are sporadic. Age is the strongest established risk factor, and researchers have also identified genetic susceptibility around the MAPT region, especially within the H1 haplotype background. Environmental triggers have been studied, but no single exposure has been accepted as a definitive cause.
Because poor balance and dysarthria are not unique to PSP, clinicians still have to distinguish it from other neurodegenerative syndromes that disrupt coordination, including ataxia. That is why disease pattern, tempo of progression, eye movement findings, and early fall history remain so important in the differential diagnosis.
Stem Cells for Progressive Supranuclear Palsy
Stem cell therapy for PSP is not appropriate or effective for all cases. Anyone evaluating regenerative options should first understand the basics about stem cell therapy, because mesenchymal cells, neural progenitors, autologous products, and allogeneic products are biologically distinct and should not be marketed as though they all work the same way[3].
In PSP, the rationale for cell therapy is usually not a simple one-for-one neuron replacement. Researchers are more interested in whether cells can reduce neuroinflammation, release neurotrophic factors, stabilize vulnerable circuits, and improve the surrounding environment for surviving cells. That is why discussions about neural stem cells, glial cells, and neurons matter here: glial support, synaptic maintenance, and paracrine signaling may be just as relevant as direct neuronal differentiation.
Manufacturing details also matter more than many marketing pages admit. Cell viability, sterility, passage number, dose consistency, release testing, and the quality of cell collection and cryopreservation can influence whether a product is even suitable for clinical use, long before anyone talks about efficacy in PSP.
Neural Stem Cell Therapy vs. Standard PSP Treatments
Standard PSP care still centers on symptom management and injury prevention. A levodopa trial is often reasonable, but the benefit is commonly limited or temporary. Other supportive options may include amantadine in selected cases, botulinum toxin for eyelid spasm or dystonia, prism lenses for difficulty with downgaze, physical therapy for balance and transfer safety, occupational therapy for daily functioning, and speech-language evaluation for communication and swallowing.
Neural cell therapy is fundamentally different in its goal. Conventional care tries to reduce day-to-day disability now, whereas regenerative protocols are marketed as attempts to modify the disease environment itself. Some programs use intravenous infusions, some discuss targeted vascular delivery, and others rely on intrathecal delivery of stem cells to place cells into cerebrospinal fluid. Those approaches are not interchangeable, and none has become a standard, guideline-supported treatment for PSP[4].
For patients and families, the practical question is not whether regenerative medicine sounds promising in theory. It is whether the proposed protocol has a defensible cell source, a clear delivery rationale, realistic goals, measurable follow-up, and a safety plan that makes sense for a fragile neurodegenerative population.
How Stem Cells May Help Address PSP Brain Injury
PSP creates a diffuse pattern of brain injury rather than a single focal defect. Damage accumulates across the midbrain, basal ganglia, and frontal networks, so a protocol designed for spinal cord injury or another focal regenerative target cannot simply be copied into PSP without major adjustments.
Theoretical mechanisms of benefit include paracrine anti-inflammatory signaling, reduced microglial activation, support of synaptic function, preservation of vulnerable neurons, and modulation of the local glial environment. Even when transplanted cells do not permanently engraft as mature neurons, they may still affect the disease milieu through secreted growth factors and immunomodulatory signals.
Ideal Candidates for PSP Stem Cell Therapy
Potential candidates for experimental PSP stem cell therapy should first have the diagnosis reviewed as carefully as possible. Screening should include a recent neurological assessment, current brain imaging, medication history, fall frequency, swallowing status, respiratory reserve, and a realistic understanding of the disease stage. The presence of a reliable caregiver also matters because PSP often affects mobility, judgment, and safe feeding long before the patient loses insight[5].
Another key question is cell source. Some programs discuss autologous cells, while others use umbilical cord-derived mesenchymal stem cells. Those cellular products are not interchangeable, and patients should know exactly which cell type is being proposed, how it was processed, and which route will be used, based on an acceptable risk profile.
Realistic treatment goals are essential. In PSP, a meaningful outcome may be fewer falls, more stable transfers, better tolerance of therapy, easier swallowing strategies, or a slower decline in functional scores. Promising a cure, full neuronal replacement, or long-term reversal of established gaze palsy would overstate the current evidence.
Post-Treatment Rehabilitation
Post-treatment rehabilitation is not optional in PSP, regardless of whether a patient receives conventional care alone or participates in an experimental cell-based protocol. Physical therapy should emphasize prevention of backward falls, cueing for turns and transfers, trunk mobility, neck extension, visual compensation strategies, and the safe use of assistive devices.
Occupational therapy helps preserve dressing, bathing, feeding, toileting, and home safety, while speech-language therapy addresses both dysarthria and dysphagia. Nutrition planning becomes increasingly important as meals take longer, fatigue worsens, and aspiration risk rises. In advanced cases, caregiver training is just as important as patient training.
TREATMENT RISKS & PRECAUTIONS
Please note that not all patients are suitable candidates for treating Progressive supranuclear palsy with stem cells. Patients with advanced motor symptoms, severe cognitive decline, or other significant health conditions might not be good candidates for treatment. The Regeneration Center does not offer embryonic stem cells or induced pluripotent stem cells for the treatment of PSPThe most useful rehab plans define objective endpoints before treatment begins. Timed mobility tests, fall counts, swallowing tolerance, speech clarity, caregiver burden, and quality-of-life measures provide a more honest picture of progress than vague impressions alone. In a disease as complex as PSP, structured rehabilitation is often the difference between theoretical improvement and meaningful daily function.
Progressive supranuclear palsy is a complex tauopathy that demands precise diagnosis, clear differentiation from Parkinsonian syndromes, and realistic expectations about what current therapies can and cannot do. Standard treatment remains supportive and symptomatic, while stem cell therapy for PSP is still in its early stages and should be viewed as an emerging treatment rather than a proven standard of care. The Regeneration Center offers balanced scientific optimism with clinical accuracy, emphasizing early recognition, multidisciplinary management, careful candidate selection, and measurable rehabilitation goals alongside any discussion of the application of regenerative medicine.
Stem Cells for PSP Treatment Guidelines
Stem Cell Treatment for Progressive Supranuclear Palsy will require an estimated two weeks in Bangkok, Thailand. Given the varying degrees of severity for this progressive, neurodegenerative condition, our medical team will need to better understand the patient’s current condition and prequalify candidates before providing treatment options. Upon approval, a detailed treatment plan will be provided, including recommendations for managing PSP diagnosis, with specifics such as the exact number of nights required in Thailand and the total medical-related costs (excluding accommodations or flights). To begin the qualification process for our multi-stage treatment protocol, please prepare your recent medical records (Biochemistry results, Genetic Tests, and Radiology scans from an MRI, CT, or PET Scans) and contact us today.
Published Clinical Citations
[1] ^ Phokaewvarangkul O, Bhidayasiri R. How to spot ocular abnormalities in progressive supranuclear palsy? A practical review. Transl Neurodegener. 2019 Jul 10;8:20. doi: 10.1186/s40035-019-0160-1. PMID: 31333840; PMCID: PMC6617936.
[2] ^ Calogero AM, Viganò M, Budelli S, Galimberti D, Fenoglio C, Cartelli D, Lazzari L, Lehenkari P, Canesi M, Giordano R, Cappelletti G, Pezzoli G. Microtubule defects in mesenchymal stromal cells distinguish patients with Progressive Supranuclear Palsy. J Cell Mol Med. 2018 May;22(5):2670-2679. doi: 10.1111/jcmm.13545. Epub 2018 Mar 4. PMID: 29502334; PMCID: PMC5908108.
[3] ^ Li H, Yuan F, Du Y, Pan T, Wen W, Li S, Wang L, Lu A. Umbilical cord blood stem cells transplantation in a patient with severe progressive supranuclear palsy: a case report. J Med Case Rep. 2021 Nov 29;15(1):574. doi: 10.1186/s13256-021-03139-z. PMID: 34844635; PMCID: PMC8628425.
[4] ^Canesi M, Giordano R, Lazzari L, Isalberti M, Isaias IU, Benti R, Rampini P, Marotta G, Colombo A, Cereda E, Dipaola M, Montemurro T, Viganò M, Budelli S, Montelatici E, Lavazza C, Cortelezzi A, Pezzoli G. Finding a new therapeutic approach for no-option Parkinsonisms: mesenchymal stromal cells for progressive supranuclear palsy. J Transl Med. 2016 May 10;14(1):127. doi: 10.1186/s12967-016-0880-2. PMID: 27160012; PMCID: PMC4862050.
[5] ^ Pezzoli G, Tesei S, Canesi M, Sacilotto G, Vittorio M, Mizuno Y, Mochizuki H, Antonini A. The effect of repeated administrations of granulocyte colony stimulating factor for blood stem cells mobilization in patients with progressive supranuclear palsy, corticobasal degeneration and multiple system atrophy. Clin Neurol Neurosurg. 2010 Jan;112(1):65-7. doi: 10.1016/j.clineuro.2009.08.023. Epub 2009 Sep 17. PMID: 19765889.