




Please complete the inquiry form below. One of our staff will contact you within 1 business day
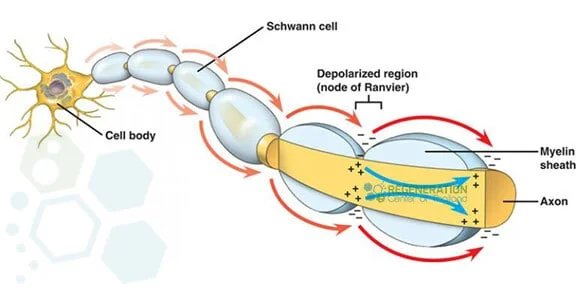
Transverse myelitis is a rare neurological impairment characterized by inflammation of both sides of the spinal cord, leading to damage to the myelin sheath, an insulating material that covers nerve cell fibers. These nerve fibers transmit motor and sensory signals to and from the brain. Myelitis refers to inflammation in the spinal cord, while transverse refers to a specific pattern of changes in sensations across the body. Symptoms of TM can be sudden (acute) or slowly develop over an extended period. [1]
TM results in a bilateral sensory deficit that can affect patients of any age, regardless of race & gender. The condition does not appear to be hereditary and is typically diagnosed in patients aged 10 to 40 years. Recovery from TM can be slow, but with early intervention and modern regenerative medicine, patients can recover from transverse myelitis with little to no lingering symptoms. If left untreated, the damage from transverse myelitis can be permanent, with impairments affecting patients’ ability to do routine daily tasks. Most patients go through a single episode of transverse Myelitis, while others can have a recurrence, especially if the patient has other underlying issues, such as autoimmune disease.
For many patients, the diagnosis of TM is idiopathic (no known cause), but for others, damage to the bundle of nerve fibers in the spinal cord can be attributed to:
For some patients, a diagnosis of transverse myelitis might be the first symptom of a completely different immune-mediated disease, such as ankylosing spondylitis. Some patients are diagnosed with “Partial” Myelitis, while others are diagnosed as “complete” due to severe numbness & paralysis on both sides of the spinal cord.
The diagnosis of transverse myelitis can be acute (sudden) or subacute (developing over 1 month). [2] The spinal cord segment where the attack occurs determines which parts of the patient’s body are affected. For some patients, damage to one segment of the spine will only affect function at that level or below, while in others, damage to myelin is localized to the nerves of the upper back and cervical spine.
Depending on age, some patients also experience frequent muscle spasms, overall discomfort, fever, headaches, respiratory problems, loss of appetite, sexual dysfunction, anxiety, chronic back pain, and depression.[3]
Treatment options for transverse myelitis depend on the patient’s age, severity, and underlying cause. Traditional treatment options aim to target the infection itself, reduce spinal cord inflammation, and manage or alleviate symptoms such as pain. Traditional management for TM and its many complications include:
For over 12 years, the Regeneration Center has been on the leading edge of functional healthcare and regenerative medical research to better understand how our immune system attacks the nerve cell fibers and myelin in patients diagnosed with autoimmune disorders. Our work focuses on using modern cell-based therapeutics to repair demyelinated spinal cords. Our research has led to a much deeper understanding of the mechanisms underlying myelin sheath damage. It offers patients a viable means to prevent and treat transverse myelitis, reduce relapse rates, and diminish harmful inflammatory activity.[4]
After an inflammatory injury, patients are left with a spinal cord injury in which the signaling capacity of nerve cells has died, resulting in loss of sensation, permanent weakness, and bladder/bowel dysfunction. The Regeneration Center has developed a novel strategy to direct stem cells into becoming healthy motor neurons. It uses proprietary developed growth factors to direct them to repair the damaged myelin sheath and reconnect with muscle fibers.
Using isolated and enhanced MSCs+ Mesenchymal cells from autologous or allogeneic sources, the Regeneration Center has successfully restored lost function in the central nervous system. This advanced treatment for TM represents a realistic option to restore some function in patients with partial paralysis.[5] MSCs+ Stem cells carry anti-inflammatory properties that help stimulate neuronal activity, regulate the immune system, and reduce the production of inflammatory proteins (associated with stress). Our combination therapy uses multipotent glial cells and neural progenitor cells to directly promote rapid axonal (nerve fiber) growth at lesion sites. MSC+ cells can differentiate into many other cell lineages, making them an attractive & non-toxic alternative to traditional treatment for Transverse Myelitis. MSC+ cells act via paracrine signaling, stimulating neurogenesis, secreting neurotrophic growth factors, modulating the plasticity of damaged tissue, restoring synaptic transmitter sites, and integrating into existing synaptic/neural networks. MSC+ stem cells also carry immunomodulatory properties that help inhibit the release of undesired pro-inflammatory cytokines.Learn more about stem cell therapies.
The treatment may also require astrocytes, Oligodendrocyte progenitor cells (OPCs), and glial cells (Glia, neuroglia), which are non-neuronal cells that help form myelin and also provide support and protection for existing healthy neurons. OPC stem cells help produce and proliferate myelin-producing oligodendrocytes needed for remyelination. They are part of an effective stem cell treatment protocol for transverse myelitis.
Type of Injections: A more aggressive combination therapy may be required for patients with acute transverse myelitis. Autologous cells might not be appropriate for all cases, and allogeneic cell infusions will require multiple infusions and will not require invasive surgery to collect cells. MSC+ cells can be delivered via a Guided Radio Scanner (when necessary) or via an intravenous drip, nebulizer, or intrathecal delivery to bypass the BBB.
Physical Rehabilitation Post-Therapy: Physical Rehabilitation therapy for TM in Bangkok is optional, depending on the patients’ travel/time constraints. Post-therapy physical rehabilitation can be provided upon request for 2-5 hours per day, up to 5 days per week. Medical visas and extended-stay accommodations for patients and families can also be included upon request.
Inflammation is a way for our bodies to protect themselves. Since the spinal cord is tightly wrapped in bony vertebrae, there is zero room for swelling or inflammation. Even a minor inflammation can exert significant pressure on the spinal cord and can damage healthy tissue surrounding the point of inflammation.
The overall success and efficacy of UC-MSC+ stem cell treatment are measured by reducing the relapse rate and total lesions 6-12 months after MSC+ treatment. The secondary outcome is achieved by accelerating recovery time, improving overall neural function, and restoring tissue. Improvements are measured using follow-up exams and radiology scans post-MSC+ Therapy.
Challenges to the effective treatment of transverse myelitis include the rapid progression of the disease and the limitations of disease-modifying drugs. Much work remains to fully understand the pathogenesis of transverse myelitis. TM affects all age groups regardless of gender, family history, or race. Some patients may require aggressive immunosuppression, but must be monitored for complications. Stem cell therapy does offer an alternative; however, early intervention with consistent physical Therapy and rehabilitation will be needed for a healthy recovery.
Due to varying degrees of existing medical conditions and the stage of inflammation, our medical team will need to review the potential candidate’s current medical condition before establishing a treatment protocol. Upon acceptance, we can provide a more accurate assessment of the patient’s condition and the outcomes we expect post-therapy. The final plan will include a daily treatment outline detailing the required days and the complete, fixed medical-related expenses (excluding accommodations or flights). Stem Cell Therapy for transverse myelitis using MSC+ cells will require a minimum of 10-16 days in Bangkok. To begin the qualification process for our multi-stage protocol, please prepare recent medical records and contact us today.
[1] ^Aungsumart, S., & Apiwattanakul, M. (2017). Clinical outcomes and predictive factors related to good outcomes in plasma exchange in severe attack of NMOSD and long extensive transverse Myelitis: Case series and review of the literature. Multiple sclerosis and related disorders, 13, 93–97. https://doi.org/10.1016/j.msard.2017.02.015
[2] ^Tradtrantip, L., Asavapanumas, N., & Verkman, A. S. (2020). Emerging therapeutic targets for neuromyelitis optica spectrum disorder. Expert opinion on therapeutic targets, 24(3), 219–229. https://bmcmedicine.biomedcentral.com/articles/10.1186/s12916-022-02482-2
[3] ^Krishnan, C., Kaplin, A. I., Deshpande, D. M., Pardo, C. A., & Kerr, D. A. (2004). Transverse myelitis: pathogenesis, diagnosis and treatment. Frontiers in bioscience : a journal and virtual library, 9, 1483–1499. https://doi.org/10.2741/1351
[4] ^Burman, J., Tolf, A., Hägglund, H., & Askmark, H. (2018). Autologous hematopoietic stem cell transplantation for neurological diseases. Journal of neurology, neurosurgery, and psychiatry, 89(2), 147–155. https://doi.org/10.1136/jnnp-2017-316271
[5] ^Lu, Z., Ye, D., Qian, L., Zhu, L., Wang, C., Guan, D., Zhang, X., & Xu, Y. (2012). Human umbilical cord mesenchymal stem cell therapy on neuromyelitis optica. Current neurovascular research, 9(4), 250–255. https://doi.org/10.2174/156720212803530708