










Please complete the inquiry form below. One of our staff will contact you within 1 business day
A stroke is an interruption of blood flow and oxygen to parts of the brain. Cell death begins once the brain’s gray matter stops receiving enough oxygen and nutrients to survive. Gray matter contains most neuronal cell bodies in the human mind. It manages many functions, including emotions, muscle control, hearing, decision-making, sensory perception, memory, speech, and self-control.
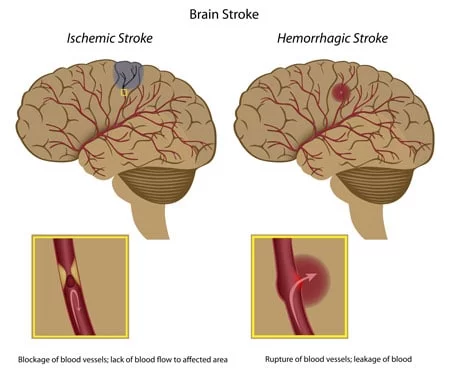
There are two main types and causes of brain strokes in the central nervous system. Sudden blocking of arteries can cause acute ischemic strokes or damage to blood vessels, resulting in bursting or leaks that can cause hemorrhagic strokes and cryptogenic strokes. Over 80-85% of strokes are ischemic, and about 10-15% of strokes are hemorrhagic. Strokes caused by bleeding cause more damage and are more challenging to treat than ischemic strokes. Some patients may have a very short disruption to the brain known as a transient ischemic attack (TIA) or “mini-stroke,” but these types of strokes are not as dangerous and might not cause permanent brain damage. Patients with chronic white-matter disease, lacunes, or microvascular injury may also need a separate review of stem cell therapy for CSVD and stroke recovery.
A stroke caused by blockage of the blood vessels that supply blood to our brain is known as an ischemic stroke and is generally the most common type of stroke we treat at the Regeneration Center. There are two main classifications for ischemic strokes.
Acute Ischemic strokes are caused by blood clots or stenosis (narrowing of the blood arteries). Stenosis is often caused by poor habits that lead to atherosclerosis, resulting in thickened, hardened, and less elastic arterial walls and decreased blood flow. Other factors include a family history of strokes/genetics, dementia, atrial fibrillation, heart disease, Congestive heart failure, diabetes, high cholesterol, and Smoking.[1]. DNA tests are now available for genetic predisposition to strokes.
A rupture in the blood vessels usually causes a hemorrhagic stroke. Several causes exist, including aneurysms, weak spots in arterial walls, and hypertension (high blood pressure). There are two main types of hemorrhagic strokes.
The severity of the physical damage caused by a stroke depends on how much blood flow was restricted and for how long. Some visible and noticeable consequences of impaired brain function are:
For most people, the symptoms of a stroke typically start without prior warning and can last from just a few seconds to a few minutes. Fortunately, patients recover quickly without further damage or issues, but this is not the case for many. The symptoms and warning signs often depend on which brain area gets affected. Severe strokes affect more significant regions in the brain; thus, more physical functions are likely lost and can result in orthopedic injuries to knees, hips, hands, or shoulders due to falls.
Currently, the only traditional treatments of ischemic strokes require restoration of proper blood flow back into the affected area by using a mechanical device or thrombolytics that physically remove any brain clots. The use of thrombolytics is very beneficial if introduced a few hours after the patient displays chronic stroke symptoms, but not very useful the longer a patient waits. This means that only a few stroke patients can take advantage of this therapy due to the timing requirements.
Several factors can increase or reduce a person’s risk of getting strokes. Some controllable risk factors for strokes include:
Other medical-related risk factors include:
Brain stroke kills twice as many women per year as breast cancer. Strokes are currently the third leading cause of death for women across the world. For this reason, women should take the necessary steps to understand the factors and make changes to reduce overall risk.
Some female-specific risk factors for having brain strokes include:
At the hospital, nerve function tests can help provide clues as to which parts of the brain are affected by the stroke and how severe the damage is. Blood collection and testing provide information on, among other things, blood counts, blood clotting, inflammatory parameters, and risk factors such as elevated cholesterol or blood glucose levels. The medical team can then use imaging techniques such as a CT Scan (computed tomography) or an MRI scan (magnetic resonance imaging) to scrutinize the patient’s brain. The radiology scans are beneficial in diagnosing whether the patient has an ischemic or hemorrhagic stroke and detecting circulatory disorders or existing cerebral hemorrhages. In addition, cerebral vessels can be visualized by CT angiography to detect blockages.
Other tests used to check the cause of the stroke and brain vessels affected by arteriosclerosis, narrowing, or thrombosis include an ultrasound or duplex sonogram. Carotid arteries are also evaluated for permeability and can be visualized with a contrast medium on CT or MRI. An electrocardiogram (ECG) is used to detect cardiac arrhythmias.
Stroke treatment depends on the type of stroke and the underlying cause. For ischemic & cryptogenic strokes, doctors need to act quickly to restore blood flow to the brain and avoid further brain damage.
Some medications for ischemic strokes can be used to try to break the clots inside the veins and must be given a few hours after a stroke.
The goal of hemorrhagic stroke treatment is to control/stop the bleeding and reduce any extra pressure on the brain. Medications for Hemorrhagic strokes include warfarin (Jantoven, Coumadin) and antiplatelet medications such as Plavix (clopidogrel) to help prevent blood clots. Note that anticoagulants and some blood thinners can interfere with stem cell therapy. Other medicines for Hemorrhagic strokes are used to lower intracranial pressure, lower blood pressure, prevent seizures, or prevent vasospasm.
Traditional treatments for stroke patients can only manage the symptoms, but cannot do much to try to repair the damaged tissue or replace the dead cells. Exosome therapy using astrocyte and neural stem cell growth factors helps target the underlying cause of the patient’s injury rather than just mask symptoms. Neural stem cell transplants are safe and painless to inject, have been shown to survive transplantation and begin differentiating into neuronal cells and new functional neurons in the brain. In addition to replacing damaged cells, replacement therapy that bypasses the blood-brain barrier can induce endogenous neural precursors that help boost the brain’s structural neuroplasticity and regulate pro-inflammatory cytokine production and the neuronal apoptotic death process. To learn about stem cells and brain-friendly diets.
Damage to the brain usually occurs when the normal flow of oxygen and blood is interrupted or blocked for a period. Getting immediate medical intervention is critical to restoring the brain’s normal blood and oxygen circulation and to avoiding long-term damage. We typically recommend having active treatments like human neural stem cell replacement as quickly as possible following a stroke to prevent the chances of lesions forming, which lead to scar tissue that cannot be repaired after a certain length of time, causing permanent paralysis with peripheral neuropathic pain in ischemic stroke patients and patients diagnosed with Complex Regional Pain Syndrome.
Neural stem cell therapy uses paracrine signaling to target the damaged neural circuitry in the brain that controls motor functions. The cells are first enhanced in our stem cell lab and then injected intravenously via a proprietary stem cell nebulizer to deliver cells near the motor neuron tracts, close to the lesions, to promote regeneration and repair through the secretion of Cytokines and nerve growth factors. The benefits are gradual; however, most patients show immediate improvement after the first or second infusions and continue to improve 3-6 months post-therapy. The results are permanent but will require consistent physical and speech rehabilitation after treatment to allow the brain to return to proper function, especially for cases with cerebral hemorrhaging and cerebral infarction.[3]
Other noticeable improvements after mesenchymal stem cell therapy for strokes include:
Mesenchymal stromal cells and isolated glial cells offer a breakthrough technology, but have limitations. Based on research and experience, the most successful patient recoveries occur when patients start pluripotent stem cell-based intervention very early after the incident. Lack of oxygen to the brain tissue can cause rapid damage and failure to other vital organs.[4] Suppose you or a loved one is unable to get stem cell therapy quickly after a stroke. In that case, we recommend daily use of hyperbaric oxygen chambers, External counterpulsation therapy (ECP), pulsed electromagnetic therapy (PEMFT) to areas on the back of the patient’s head, neural growth factors, nutritional IV injections, and periodic acceleration therapy.
Brain stroke can lead to severe brain tissue damage, resulting in permanent paralysis for some patients. Neural stem cell therapy for strokes has limitations but offers a viable potential cure for paralysis caused by brain infarction. There is clinical trial evidence that shows neurogenic endogenous stem cells & multipotent adult progenitor cells transplanted into the brain can initiate repair and related events, reaching peak levels, suggesting that exogenous cell therapies can indeed regenerate damaged brain tissue and help promote functional recovery in some stroke patients.
Pluripotent stem cell therapies offer a promising way to regenerate neurons damaged by a brain stroke. Stem cell research has shown that isolated and expanded UC-MSC+ cells rapidly promote functional recovery in stroke patients by reducing the severity of brain damage after infarction. These cultured stem cells release growth factors that promote the development of new blood vessels (angiogenesis), reduce systemic inflammation, and aid in the regeneration of damaged brain tissue.
Physical and Speech Rehabilitation is highly recommended after a stroke treatment and can be provided at a local hotel facility upon request. We can also assist you in finding certified physical or speech rehabilitation with an accredited therapist in your home country, depending on where you live. Medical visas and accommodations for an extended stay at serviced apartments are provided upon request.
Due to varying severity, our medical team must review the patient’s medical records and diagnostic imaging results. Once the medical review is complete, we can determine whether the patient is a good candidate and provide a fixed cost for the treatment. To help us make an accurate assessment and provide a detailed treatment plan, our medical staff will need to review the recent medical records, including any imaging results from Brain radiology scans. (Test Results less than three months old are required for treatment evaluation.)
To begin the medical evaluation for our multi-stage stroke treatment, please contact us today.
[1] ^ Bandasak, Ratanaporn, Kulaya Narksawat, Chanpong Tangkanakul, Yotin Chinvarun, and Sukhontha Siri. 2011. Association between hypertension and stroke among young Thai adults in Bangkok, Thailand. The Southeast Asian journal of tropical medicine and public health, no. 5. https://www.ncbi.nlm.nih.gov/pubmed/22299451
[2] ^ Nilanont, Yongchai, Samart Nidhinandana, Nijasri C Suwanwela, Suchat Hanchaiphiboolkul, Taksin Pimpak, Pyatat Tatsanavivat, Gustavo Saposnik, and Niphon Poungvarin. 2013. Quality of acute ischemic stroke care in Thailand: a prospective multicenter countrywide cohort study. Journal of stroke and cerebrovascular diseases : the official journal of National Stroke Association, no. 2 (January 8). doi:10.1016/j.jstrokecerebrovasdis.2012.12.001. https://www.ncbi.nlm.nih.gov/pubmed/23305673
[3] ^ Dharmasaroja, Permphan. 2008. Bone marrow-derived mesenchymal stromal stem cells for the treatment of ischemic stroke. Journal of clinical neuroscience : official journal of the Neurosurgical Society of Australasia, no. 1 (November 18). doi:10.1016/j.jocn.2008.05.006. https://www.ncbi.nlm.nih.gov/pubmed/19017556
[4] ^ Hao, Lei, Zhongmin Zou, Hong Tian, Yubo Zhang, Huchuan Zhou, and Lei Liu. 2014. Stem cell-based therapies for ischemic stroke. BioMed Research International (February 26). doi:10.1155/2014/468748. https://www.ncbi.nlm.nih.gov/pubmed/24719869