






Please complete the inquiry form below. One of our staff will contact you within 1 business day
The Regenerative Centers’ orthopedic stem cell protocols offer a safe and effective alternative to hip replacement surgery for treating degenerative hip conditions, injuries & arthritis. Our non-surgical stem cell-based treatment is a true breakthrough for millions of men and women needlessly suffering from chronic hand, wrist, knee injuries, knee arthritis, and hip pain due to a variety of reasons, such as: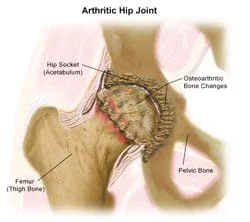
Our hip and shoulder stem cell therapies are combined with enriched blood PRP (platelet-rich plasma) and growth factors to allow an effective and 100% non-surgical solution for our patients with cartilage damage, DDD, Spinal Injuries, moderate femoral nerve pain, or who may be considering hip replacement surgery or hip resurfacing to try to resolve the chronic hip pain.[1] Our treatment protocol is ideal for mild and moderate cases of ligament cartilage damage and for those who want to regenerate/reverse hip problems without surgery using enriched lab concentrated mesenchymal cell injections using the patient’s stem cells (autologous– for mild conditions ) or immunosystem matched allogeneic stem cells( for moderate to severe conditions) This unique protocol allows our orthopedic stem cell doctors to target the problem at the root and treat it using enriched tissue manipulation techniques that will enable treated arthritic knees and hips to heal themselves without the need for invasive surgery naturally.[2]
Hip surgeries, such as replacement and resurfacing, are typically invasive and often cause months of postoperative pain and discomfort, especially during rehabilitation to rebuild strength and restore mobility in the hip socket and joint spaces disrupted by mild osteoarthritis.[3]
Our orthopedic stem cell hip treatment works by targeting the areas of arthritis or injury with both clinical-grade stem cells and ( PrP ) platelet-rich plasma. Cultured stem cells and paracrine cell signaling act as biological seeds, with tissue-specific growth factors that serve as fertilizers to strengthen cells and help quickly heal injured areas. Our unique 2-week treatment course uses isolated stem cells with Transforming Growth Factor-Beta (TGF-β) growth factors, Platelet-Derived Growth Factor (PDGF), Bone Morphogenetic Proteins (BMPs), Vascular Endothelial Growth Factor (VEGF), and Fibroblast Growth Factor (FGF), which are delivered to the patient on alternative cell infusion dates via the blood circulatory system. Unlike most 1-3-day treatments, these additional steps in our treatment protocol enhance cell signaling and provide essential signals and nutrients that support orthopedic stem cells to flourish across multiple life cycles. This additional step helps develop the introduced cells into new, healthy joints, tendons, and ligaments. The Regeneration Center uses a proprietary closed-system UC-MSC+ cell culture to promote rapid stem cell development.
Regenerative medicine is a conservative treatment option and might not be the final answer for all patients with degenerative hip injuries and neuropathy. However, most sports medicine cases treated with UC-MSC+ stem cells are successful in the long term and help our patients improve their quality of life, avoid pain, downtime, and disability, and, most importantly, the risks associated with major surgery such as total hip replacement. Our bone regeneration protocols are minimally invasive, and recovery time is minimal after treatment. Most patients report only slight soreness in the treated areas, with minimal bruising, for 24-48 hours post-therapy. Our center has never had any patients experience adverse effects, as all cells are tested and certified before implantation. After hip joint treatment, patients are encouraged to follow a hip osteoarthritis diet and engage in regular hip rehabilitation to help restore proper hip function. Hip stem cell treatments offer a viable alternative and are very safe to try, even for severe cases. Stem cell therapies using cells from your own body can also be repeated after 6-12 months (if necessary) to achieve optimal results for people with active lifestyles. For patients with severe hip damage, stem cell treatment alone might not be sufficient. For cases requiring core decompression or severe musculoskeletal conditions, we offer a unique treatment that combines microsurgery with stem cells (administered after surgery) and cell-specific growth factors to expedite and normalize the healing process, leading to faster recovery and a lower risk of scarring or hip arthritis.
Number of Cell Infusions for Hip arthritis and hip pain: 2-8 Targeted infusions of expanded Mesenchymal “UC-MSC+” Cells with tissue-specific growth factors for increasing formation of fibrocartilage fibers, growth factors & differentiated scaffolds.
Types of Stem Cells and Delivery Methods for Hip: Enhanced UC-MSC+ Mesenchymal cells & Hip regenerative therapy protocol will depend on the severity of the underlying degeneration, as needed. Our cell-enriched treatments do not require any invasive surgeries. The delivery of the cells is made via radio guidance (when necessary) or, more commonly, through the combination of Intravenous Drip, direct Local injections, Intra-articular Injections, Intraosseous Injections, Intrathecal Injections (if experiencing neuropathy), Ultrasound-guided (in office) or fluoroscopy-guided stem cell delivery (in a hospital setting only).
Rehabilitation Options Post-Treatment: Physical rehabilitation therapy is strongly recommended after treatment and can be provided in Thailand or upon return home. We offer optional in-person rehab packages based on your travel/time constraints. Our physical therapy and pain relief programs are available upon request for 2-3 hours per day and up to 5 days per week. Medical visas and hotel accommodations for the patient and family can also be provided upon request.
Total Treatment Length: The estimated treatment time for stem cell therapy for hip pain and degenerative hip arthritis is 10-14 days in Bangkok (depending on the severity of the underlying injury)
The Regeneration Center offers patients a cohesive & comprehensive approach to hip joint injuries that yields the most beneficial results possible without the risks of hip replacement surgeries. We have treated professional athletes to average elderly patients who needlessly suffered through decades of chronic hip joint pain. If you or a loved one is suffering from a degenerative hip condition or chronic hip pain, or if you have any difficulty standing up or walking stairs, you may be a candidate for our procedure. To learn more, please contact us today.
Due to the varying degrees of injuries, our orthopedic team must conduct a medical review of all potential patients. This can be done online using the patient’s current medical records, such as Hip MRI or CT Scan, and reports from the patient’s orthopedic doctors. Once the treatment evaluation is complete, we can determine whether the patient is a good candidate and provide a detailed treatment plan with the total number of stem cell injections, the number of nights required, and fixed medical-related costs for the entire treatment.
[1] ^ Homma, Yasuhiro, Kazuo Kaneko, and Philippe Hernigou. 2013. Supercharging allografts with mesenchymal stem cells in the operating room during hip revision. International orthopaedics, no. 10 (December 10). doi:10.1007/s00264-013-2221-x. https://www.ncbi.nlm.nih.gov/pubmed/24323352
[2] ^ Houdek, Matthew T, Cody C Wyles, John R Martin, and Rafael J Sierra. 2014. Stem cell treatment for avascular necrosis of the femoral head: current perspectives. Stem cells and cloning : advances and applications (April 9). doi:10.2147/SCCAA.S36584. https://www.ncbi.nlm.nih.gov/pubmed/24744611
[3] ^ Rungsiyanont, Sorasun, Nirada Dhanesuan, Somporn Swasdison, and Shohei Kasugai. 2011. Evaluation of biomimetic scaffold of gelatin-hydroxyapatite crosslink as a novel scaffold for tissue engineering: biocompatibility evaluation with human PDL fibroblasts, human mesenchymal stromal cells, and primary bone cells. Journal of biomaterials applications, no. 1 (February 22). doi:10.1177/0885328210391920. https://www.ncbi.nlm.nih.gov/pubmed/21343214