





Please complete the inquiry form below. One of our staff will contact you within 1 business day
Spinal Stenosis is a medical condition characterized by the narrowing of the spinal canal, which results in increased pressure on the spinal cord and nerve roots. This condition can be congenital or develop over time due to age-related changes in the spine, such as bone spurs and thickened ligaments. Depending on where it occurs, it can cause pain, numbness, and weakness in various body parts.
The most common symptoms associated with spinal Stenosis include pain and numbness along the back or legs that worsens with standing or walking and is relieved after sitting down or leaning 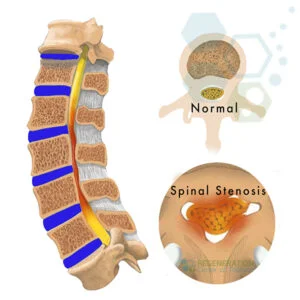
Potential causes of spinal Stenosis can include other age-related changes like herniated discs, arthritis formation within joints, thickening of ligaments, a buildup of bony growths (bone spurs) that pinch nearby nerves, trauma such as an injury causing misalignment in vertebrae, which can decrease available space, or diseases like Paget’s disease, which involves excessive bone growth. Additionally, tumors and cysts may reduce the space available for nerve pathways within the spine.
Symptoms of spinal stenosis can vary depending on the severity of the condition and where it is located. Some common symptoms include pain in the lower back, buttocks, or thighs; cramping in the legs or arms; weakness or numbness in the legs, arms, hands, or feet; tingling sensation in the back or extremities; difficulty walking for long distances; balance issues, such as feeling unsteady when turning or bending.
Potential causes of Spinal Stenosis include bulging discs, bone spurs (osteophytes) developing on either vertebral facet joints, hypertrophy of surrounding ligaments like the supraspinous ligament, and intraspinal enlargements from tumors or nerve entrapment. In addition to these causes specifically causing spinal stenosis, other conditions like sarcopenia, osteoarthritis, and lumbar spondylolisthesis have been linked with stenosis development through their mechanical effects on nerves [2].
When the spinal canal narrows, it may compress the spinal roots or femoral nerves, resulting in pain. Causes for a diagnosis can vary greatly, ranging from genetics to activity level to age-related wear and tear. Other potential risk factors for spinal Stenosis include previous injuries (especially from a fall), ankylosing spondylitis, metabolic diseases, diminishing bone density as we age (osteoporosis), scoliosis, arthritis, tumors, and viral or bacterial infections such as Lyme disease. A history of being born with a congenitally narrow spinal canal is also associated with a higher risk of developing the condition later in life.
Diagnosis of spinal stenosis in the cervical (neck) or lumbar (lower back) region can be made through various means, including physical examination, imaging (CT and MRI), myelography, electrophysiological studies (nerve conduction tests), and musculoskeletal testing. During the initial physical examination, your orthopedic doctor may check the limbs for reflexes and strength. Patients are tested by performing simple neurological tasks. Imaging scans are also used to identify bone structure compression or narrowing. Types of radiologic imaging include X-rays, MRI, CT, and Ultrasound. MRI scans provide cross-sectional images using magnetic fields and radio waves.
In some cases, a myelogram may also be ordered, requiring contrast dye to determine if there are any blockages in the area. Non-invasive electrical studies and nerve conduction tests can be used to assess how well nerves respond to stimuli. At the same time, biochemical tests can assess for evidence of infection or inflammation, as secondary infections have been associated with spinal stenosis.
Depending on the stage and severity, physicians may recommend lifestyle modifications, such as physical therapy, to enhance overall strength and flexibility and reduce spinal inflammation. Nonsteroidal anti-inflammatory drugs (NSAIDs) may be prescribed to help reduce pain and swelling for patients. Steroids may be used if more severe inflammation is present, accompanied by spasms in the surrounding muscles. In some cases, surgery may be recommended to increase available nerve pathways, thereby alleviating pressure caused by spinal Stenosis. Surgery may require rods or screws combined with fused vertebrae sections.
Surgical treatment options may include:
For many patients, stem cell therapy offers a non-surgical alternative to treat degenerative discs and spinal stenosis, and has been proven to show improvements in several areas. Depending on patient needs, stem cells from different sources (autologous vs. allogeneic) have varying degrees of effectiveness in promoting differentiation and producing desired biological effects. Since 2007, The Regeneration Center has developed a deep understanding of stem cell therapies for low back pain (LBP), Intervertebral disc degeneration (IDD), acute spinal injuries, spinal stenosis, and intervertebral disc herniation.
Isolated and expanded stem cells have been used to intervene in spinal stenosis and inflammation to help slow down progression, boost stem cell production, and achieve repair through cell regeneration. The Regeneration Medical Center currently offers several types of cell therapies, including:
The three primary functions of regenerative stem cells are:
Types of Stem Cells and Delivery Methods: Multiple Sessions of Enhanced UC-MSC+ Mesenchymal Cells & spinal regenerative therapy protocol will depend on the underlying stage’s severity and the patient’s condition. Our clinical-grade lab cell-enriched allogeneic cell protocols cells do not require any invasive surgeries. The cells are delivered via intravenous drips, direct local injections, intradiscal injections, intrathecal injections, fluoroscopy-guided stem cell delivery (in a hospital setting only), or a combination of different delivery methods to achieve the best results. To learn about the basics of stem cells, visit here[5].
Safety and efficacy are as important as results; therefore, our unique multi-stage cellular therapy for spinal stenosis will require 1-2 Weeks in Bangkok, Thailand. Given the varying degrees of spinal damage among patients, our orthopedic team will need to evaluate potential candidates. Upon completion of the evaluation, a detailed treatment plan will be provided. It will include specific recommendations, such as a day-by-day treatment calendar (appointment dates), the total number of nights required, and fixed medical costs (excluding accommodations or flights). To begin the treatment evaluation, please prepare recent medical records, such as MRI or CT Scans, and contact us today.
Post-Treatment Physical Rehabilitation & Pain Relief: For patients with Cervical Stenosis with myelopathy, Ankylosing spondylitis (spinal stenosis), or osteoporosis, physical rehabilitation after treatment is optional, depending on travel limitations. Total post-therapy rehab plans are also available for 2-4 hours per day and up to 5 days per week. We also offer comprehensive regenerative medicine packages, assistance with medical visas, and extended-stay accommodations for the patient and family upon request.
[1] ^Kasai Y, Paholpak P, Wisanuyotin T, Sukitthanakornkul N, Hanarwut P, Chaiyamoon A, Iamsaard S, Mizuno T. Incidence and Skeletal Features of Developmental Cervical and Lumbar Spinal Stenosis.Intermittent Neurogenic Claudication Asian Spine J. 2022 May 10. doi: 10.31616/asj.2022.0015. Epub ahead of print. PMID: 35527532.
[2] ^Lee JY, Whang PG, Lee JY, Phillips FM, Patel AA. Lumbar spinal stenosis. Instr Course Lect. 2013;62:383-96. PMID: 23395043.
[3] ^Chaimongkhol T, Thiamkaew A, Mahakkanukrauh P. The characteristics of osteophyte around lumbar vertebral foramina associated with spinal stenosis. Anat Cell Biol. 2019 Jun;52(2):143-148. doi: 10.5115/acb.2019.52.2.143. Epub 2019 Jun 30. PMID: 31338231; PMCID: PMC6624344.
[4] ^ Vadalà G, Ambrosio L, Russo F, Papalia R, Denaro V. Stem Cells and Intervertebral Disc Regeneration Overview-What They Can and Can’t Do. Int J Spine Surg. 2021 Apr;15(s1):40-53. doi: 10.14444/8054. Epub 2021 Apr 21. PMID: 34376495; PMCID: PMC8092931.
[5] ^ Sivakamasundari V, Lufkin T. Stemming the Degeneration: IVD Stem Cells and Stem Cell Regenerative Therapy for Degenerative Disc Disease. Adv Stem Cells. Halo Vest vs. Spinal Fusion 2013;2013:724547. doi: 10.5171/2013.724547. PMID: 23951558; PMCID: PMC3742038.