






Please complete the inquiry form below. One of our staff will contact you within 1 business day
A diagnosis of Cerebral Small Vessel Disease (CSVD), also called chronic small vessel disease or white matter disease, can be confusing and concerning for patients and families. In many cases, CSVD is discovered after a brain MRI or CT scan shows white matter changes, lacunar infarcts, microbleeds, or signs of long-term injury to the brain’s smallest blood vessels. Some patients have no obvious symptoms at first, while others may experience memory changes, slower thinking, balance problems, walking difficulty, mood changes, fatigue, or stroke-like neurological deficits.[1]
Because CSVD affects the small vessels that support the brain’s deep white matter and delicate neural networks, treatment is usually focused on protecting the brain from further vascular injury. The established foundation of care is careful control of risk factors such as high blood pressure, T1 Diabetes, cholesterol imbalance, smoking, sleep apnea, inflammation, and other conditions that can damage the microcirculation over time.
Stem cell and cell-based approaches for CSVD remain investigational and should not be viewed as a cure or a replacement for standard neurological and vascular care. At The Regeneration Center, our approach is a supportive, regenerative protocol for carefully selected patients. The goal is to address several biological processes that may contribute to CSVD progression, including chronic inflammation, endothelial dysfunction, impaired microcirculation, oxidative stress, and reduced neurovascular repair capacity.
Depending on the patient’s diagnosis, imaging findings, neurological symptoms, vascular risk profile, and overall medical condition, our medical team may consider a personalized protocol using umbilical cord-derived mesenchymal stem cells, supportive growth factors, anti-inflammatory and vascular-supportive therapies, and rehabilitation-focused planning. While outcomes cannot be guaranteed, the right patient may benefit from a comprehensive evaluation to determine whether regenerative support is appropriate as part of a broader, medically supervised care strategy. Our aim is to provide accurate, balanced information so patients and families can better understand CSVD, prepare the correct medical records, and decide whether a specialist evaluation is the right next step.
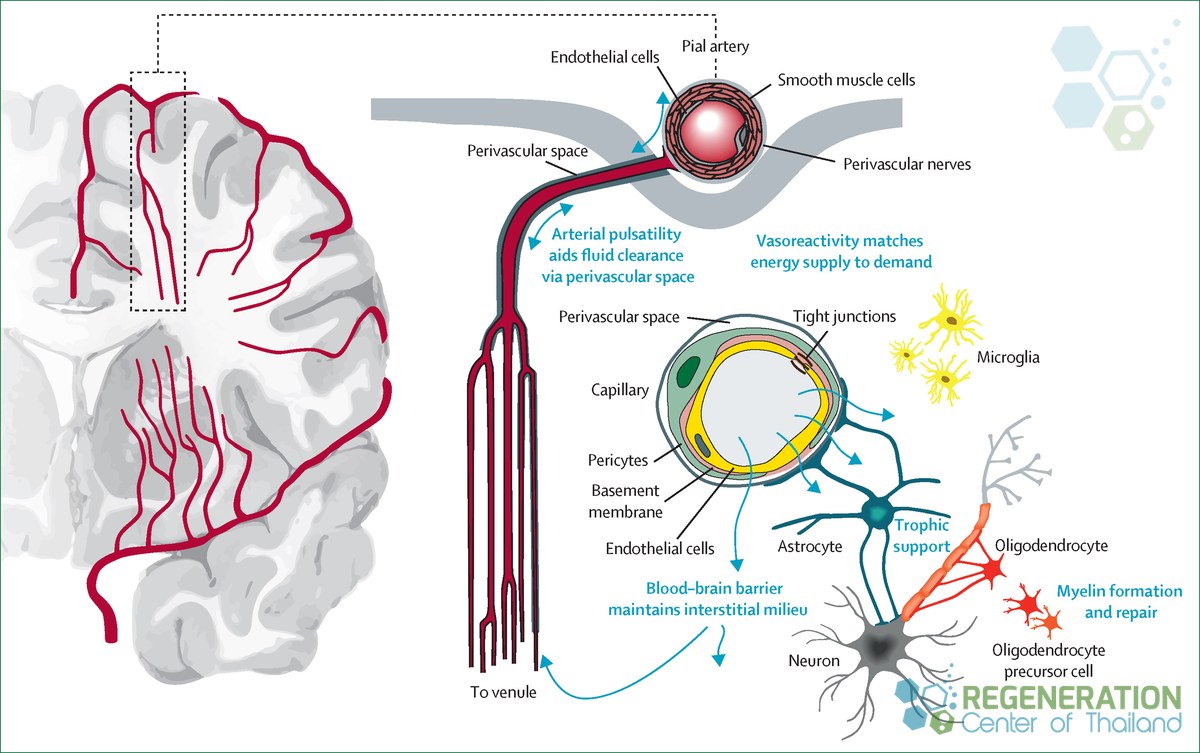
Cerebral small vessel disease is an umbrella term for damage to the brain caused by problems in its smallest blood vessels: the tiny arteries, arterioles, and capillaries that supply deep brain tissue. When these vessels stiffen, narrow, or leak over time, the surrounding tissue receives less reliable blood flow. The result is a slow, often quiet form of injury that builds up over the years.[2]
CSVD matters because it is common with age and because it sits behind two serious problems: stroke and cognitive decline. One widely cited review reports that CSVD contributes to roughly 20 percent of strokes and to a large share of dementias. It is a leading driver of the kind of memory and thinking changes that lead to a diagnosis of vascular dementia, and it is closely linked to lacunar and ischemic stroke recovery. Public health agencies describe vascular factors as a major contributor to cognitive impairment, second only to Alzheimer’s disease, which is part of why CSVD has become a research priority.
The terminology can be confusing, since radiologists and neurologists use several overlapping words. You may see “leukoaraiosis,” “white matter changes,” “chronic microvascular ischemia,” or “small vessel ischemic disease” in a report. These generally point to the same underlying process. If a term in a medical letter is unfamiliar, the regenerative medicine glossary can help translate it.
CSVD injures the brain through several recognizable patterns that doctors look for on scans. Each reflects a different way small-vessel damage manifests in tissue.
A common thread across these findings is the breakdown of the blood-brain barrier, the tightly controlled lining that normally keeps blood and brain tissue separate. When that barrier becomes leaky, fluid and harmful molecules can reach protected tissue, and waste clearance can suffer. Over time, this contributes to the loss of white matter integrity that underlies many CSVD symptoms.
Radiologists sometimes grade the extent of white matter change using standardized scales, and they often compare scans from different time points to assess whether the disease is progressing. This is one practical reason to keep copies of imaging and reports, since change over time is easier to interpret when earlier studies are available for comparison.[3]
This slow, diffuse pattern is different from a single dramatic event. It is worth distinguishing CSVD from sudden conditions such as hypoxic and acquired brain injury, where damage happens quickly and from a clear cause. CSVD tends to accumulate, which is part of why it can remain undetected for a long time.
Many people with early CSVD have no obvious symptoms, and the disease is often found by chance when a brain scan is done for another reason. As changes accumulate, symptoms can appear gradually and may be mistaken for ordinary aging.
Diagnosis rests mainly on brain imaging. Magnetic resonance imaging (MRI) is the most informative test, because it shows white matter hyperintensities, lacunes, and microbleeds far better than a standard CT scan. Doctors usually combine imaging with a medical history, a cognitive assessment, and a review of vascular risk factors such as blood pressure, cholesterol, and blood sugar. For families comparing different conditions, the center groups related diagnoses under neurological and spinal conditions, which can help put a CSVD diagnosis in context.
The established treatment for CSVD focuses on controlling the vascular risk factors that drive small-vessel damage. There is no medication that has been shown to repair existing damage, so the priority is to slow further injury and lower the risk of stroke and decline.
European Stroke Organization guidelines, which represent current expert consensus, place the strongest emphasis on blood pressure management. People with CSVD and high blood pressure should have it well controlled, and lower targets may slow disease progression. The same guidance notes that routine antiplatelet drugs such as aspirin are not recommended for covert CSVD found incidentally on imaging, which is an important point because it differs from how some other vascular conditions are managed. Decisions about medication should always be made with the treating physician.
Because CSVD shares risk factors with the rest of the cardiovascular system, good general health care matters. Managing ischemic heart disease, keeping type 2 diabetes under control, and protecting kidney health in people with chronic kidney disease all support the same small vessels. Lifestyle measures carry real weight too. Guidelines highlight smoking cessation as a health priority and support regular exercise, a healthy diet, adequate sleep, and the avoidance of obesity. For people who have had a lacunar stroke, secondary prevention follows established stroke-prevention practice.
Acting early tends to matter more than acting dramatically. Because CSVD accumulates quietly, steady management over months and years usually does more to protect the brain than any single intervention. Regular review with a physician allows treatment to be adjusted as blood pressure, cholesterol, and other measures change, and it gives the care team a chance to catch new symptoms before they progress. Risk-factor control is the part of CSVD care with the clearest evidence, and any discussion of treatment options should sit alongside it rather than replace it.
Researchers are interested in cell-based approaches because risk-factor control, while essential, does not undo damage that has already occurred. As one 2024 review put it, controlling risk factors alone has not been enough to halt the progression of CSVD brain injury, which has prompted interest in strategies aimed at the underlying tissue.4 This is a research rationale, not a demonstrated treatment.[4]
Most attention has focused on mesenchymal stem cells, a type of adult stromal cell that can be obtained from sources such as umbilical cord tissue, bone marrow, or adipose tissue. Importantly, the interest in these cells is not based on the idea that they turn into new brain cells in large numbers. Instead, the leading hypothesis is that they may act through signaling.
The proposed mechanisms, which have been studied in the laboratory and used in the Regeneration Center Protocol, include several distinct processes that should not be assumed to all work together in patients:
These ideas are biologically reasonable and are an active area of study. They are also, at present, hypotheses and preclinical findings rather than confirmed clinical effects.
The scientific interest in regenerative and cell-based approaches for Cerebral Small Vessel Disease (CSVD) is growing, but it is important to understand where the evidence currently stands. CSVD is a complex condition involving the brain’s smallest blood vessels, chronic inflammation, endothelial dysfunction, changes in the blood-brain barrier, impaired microcirculation, oxidative stress, and gradual injury to white matter pathways. Because of this complexity, we are actively studying several therapeutic directions that may help protect or repair the neurovascular system over time.
At this stage, stem cell treatment for CSVD should still be considered investigational. We have had encouraging results in several cases, but results vary due to the age of the diagnosis and ongoing vascular brain injury, stroke, neuroinflammation, endothelial function, and other neurological conditions. The most established medical strategy remains careful control of vascular risk factors such as high blood pressure, diabetes, cholesterol imbalance, smoking, sleep apnea, and other conditions that can continue to damage the small vessels of the brain.
Cell-based therapies for CSVD-like conditions can provide benefits through a combination of intrathecal and intravenous infusions of UC mesenchymal stem cells, which were associated with improved cognitive performance and signs of blood-brain barrier repair via remodeling of small vessels.5 Neural progenitor cells and mesenchymal stem cells can help reduce amyloid-beta deposition and ease neuroinflammation. Our early findings cannot guarantee a cure, but targeted regenerative approaches can influence several biological pathways relevant to CSVD, including inflammation, vascular repair, and neurovascular support.
Our experience in related areas, including strokes, vascular cognitive impairment, endothelial dysfunction, and inflammatory neurological disease, is also helping us better understand how the brain’s vascular and immune systems may respond to regenerative or biologically active therapies. Findings from related neurological conditions, such as stroke or multiple sclerosis, cannot be directly applied to CSVD without caution, but they do provide useful background for understanding the mechanism of improvements. Clinical trials are also testing non-cell-based approaches targeting small-vessel function and endothelial health, including an endothelial-targeted study for CSVD that is currently underway. Patients and families who want to better understand the broader research landscape can also review our summaries of published results from stem cell clinical trials.
The Regeneration Center is not a clinical trial site for CSVD, and treatment at our center should not be confused with enrollment in a formal research study. We are a private medical treatment center that evaluates each patient individually and uses a proprietary, physician-guided regenerative protocol tailored to the patient’s diagnosis, imaging findings, neurological symptoms, vascular risk factors, and overall health status. For selected patients, our goal is to provide supportive regenerative care that may help address inflammation, microvascular dysfunction, endothelial stress, and impaired repair signaling while working alongside, not replacing, standard neurological and vascular management.[5]
It is also worth noting where treatment options are heading. Some of our research has shifted toward the biologically active molecules released by cells rather than the cells themselves, including extracellular vesicles and expanded exosomes with tissue-specific growth factors. These are not stem cells, but they may help explain some of the signaling effects being studied in regenerative medicine. For CSVD specifically, this work is still early but reflects a broader scientific direction: future treatment strategies for CSVD may involve protecting small vessels, reducing inflammation, improving endothelial function, and supporting the brain’s natural repair environment, rather than relying on a single intervention.
Candidacy for any regenerative program depends on individual medical review, not on a fixed checklist. A careful evaluation considers the diagnosis, the current state of the disease, other health conditions, and what the person and family hope to achieve. Some people are not suitable candidates, and a responsible evaluation will say so when that is the case. Factors such as the stage of disease, the stability of blood pressure and other conditions, and a person’s overall health all feed into that judgment, which is why a thorough review of records comes before any discussion of a specific plan.
If you decide to request a review, gathering records in advance will make the process more effective. Helpful information usually includes:
You can read more about our general philosophy and approach to stem cell treatments. The Regeneration Center primarily works with mesenchymal cells, with the specific plan determined on a case-by-case basis after medical review. Details such as cell source, delivery method, number of visits, and any rehabilitation support are decided individually based on the patient’s medical needs and must be confirmed by our medical team.
Cell therapy for CSVD is not an appropriate treatment for all patients, and results can vary from patient to patient. After the initial evaluation, we will define measurable markers and track them honestly over time, so that any change, or lack of change, is documented rather than assumed.
Outcomes that can actually be measured include:
Depending on the patient’s condition, having realistic expectations is essential. Responses vary among individuals, and for CSVD, the current evidence is insufficient to estimate the likelihood of any benefit or its magnitude. The same caution applies to many neurological conditions in which regenerative approaches are studied, from Parkinson’s disease to peripheral neuropathy. Honest measurement, paired with continued risk-factor control and rehabilitation, is the most useful way to understand whether anything is helping. Physical therapy, speech therapy, and cognitive support are not afterthoughts; for many people, they yield the most noticeable day-to-day gains and remain valuable regardless of whether an experimental option is pursued.
If you would like an informed opinion on whether regenerative options are worth considering, the most practical step is to have your medical records reviewed. This is a chance for the medical team to review the diagnosis, imaging, and history and provide a candid assessment rather than a sales pitch.
Gathering the records listed above before you reach out will make the review more accurate. There is no need to rush a decision, and a good evaluation should leave you better informed about whether treatment is appropriate. When you are ready, you can request a medical evaluation and share the relevant documents for review.
Whatever you decide about experimental options, continuing established care for cerebral small vessel disease remains important. Blood pressure control, healthy habits, and regular specialist follow-up are the measures with the clearest evidence, and they support the brain’s small vessels every day.
[1] ^Thiankhaw K, Panteleienko L, Stewart CR, Oliver R, Mallon D, Ambler G, Werring DJ. Association of Intracranial Dolichoectasia and Cerebral Small Vessel Disease in Patients With Intracerebral Hemorrhage. J Am Heart Assoc. 2025 Jun 17;14(12):e039039. doi: 10.1161/JAHA.124.039039. Epub 2025 Jun 11. PMID: 40497512; PMCID: PMC12229135.
[2] ^ Pasi M, Sugita L, Xiong L, Charidimou A, Boulouis G, Pongpitakmetha T, Singh S, Kourkoulis C, Schwab K, Greenberg SM, Anderson CD, Gurol ME, Rosand J, Viswanathan A, Biffi A. Association of Cerebral Small Vessel Disease and Cognitive Decline After Intracerebral Hemorrhage. Neurology. 2021 Jan 12;96(2):e182-e192. doi: 10.1212/WNL.0000000000011050. Epub 2020 Oct 16. PMID: 33067403; PMCID: PMC7905779.
[3] ^ Kim SE, Kim HJ, Jang H, Weiner MW, DeCarli C, Na DL, Seo SW. Interaction between Alzheimer’s Disease and Cerebral Small Vessel Disease: A Review Focused on Neuroimaging Markers. Int J Mol Sci. 2022 Sep 10;23(18):10490. doi: 10.3390/ijms231810490. PMID: 36142419; PMCID: PMC9499680.
[4] ^Voesenek BJB, van der Graaf LM, Lesnik Oberstein SAJ, van Roon-Mom WMC, Daoutsali E, Buijsen RAM. Generation of 4 human induced pluripotent stem cell lines (LUMCi070-A, -B, -C, and -D) from a patient with ischemic cerebral small vessel disease. Stem Cell Res. 2026 Jun 14;95:104036. doi: 10.1016/j.scr.2026.104036. Epub ahead of print. PMID: 42296843.
[5] ^ Chen DH, Huang JR, Su SL, Chen Q, Wu BY. Therapeutic potential of mesenchymal stem cells for cerebral small vessel disease. Regen Ther. 2024 Feb 22;25:377-386. doi: 10.1016/j.reth.2023.11.002. PMID: 38414558; PMCID: PMC10899004.